
Translate this page into:
Benign prostatic hyperplasia treated with individualised homoeopathic medicines: An evidence-based case series

*Corresponding author: Dr. Bikash Biswas, Department of Case Taking and Repertory, Mahesh Bhattacharyya Homoeopathic Medical College and Hospital, Howrah, West Bengal, India. bikash21592@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Biswas B, Mandal S, Abbas J. Benign prostatic hyperplasia treated with individualised homoeopathic medicines: An evidence-based case series. J Intgr Stand Homoeopathy 2022;5:99-106.
Abstract
The study aimed to evaluate the effects of homoeopathic treatment in patients with benign prostatic Hypertrophy (BPH). This was an experimental study conducted using the primary data and assessed based on clinical symptoms and pathological reports. A total of three cases were included in this study. BPH was diagnosed based on clinical symptoms and ultrasonography reports. The patients were prescribed Lycopodium clavatum, Thuja occidentalis and Arsenicum album based on clinical signs, the totality of symptoms and individualisation. Dietary changes were recommended as well. Improvement was assessed based on symptom reduction and changes in ultrasonography reports. All three patients improved clinically and pathologically, including a reduction in prostate size. This case series provides evidence that individualised homoeopathic treatment is effective in pathological conditions such as BPH, in both symptom relief and pathological changes.
Keywords
Benign prostatic hypertrophy
Individualization
Homoeopathy
Repertory

INTRODUCTION
The prostate gland is a part of the male reproductive system, located between the bladder and the penis. The male urethra passes through the centre of the prostate. The primary function of the prostate is secreting fluid that protects and nourishes the sperm in the semen.[1]
Benign prostatic hypertrophy (BPH) is a non-neoplastic tumour-like enlargement of the prostate gland.[1] BPH is one of the most common problems in older men. The common symptoms of BPH are Moderate-to-severe lower urinary tract symptoms such as urinary urgency, frequency, incomplete bladder emptying, the intermittent flow of stream and nocturia.[2] While BPH is benign, it significantly affects the day-to-day activities and the quality of life and, therefore, should not be ignored or underestimated.[3] For clinical diagnosis, at least two of the following features must be present: Urinary tract symptoms as described above, an International Prostate Symptom Score (IPSS) of more than 8, total prostatic volume >30 mL and maximum urinary flow rate (Qmax) <15 mL/sec.[4] Modern medicine prescriptions for treating BPH include alpha-blockers and 5-alpha reductase inhibitors.[5-7] Surgical procedures such as transurethral laser ablation of the prostate and transurethral resection of the prostate are available, but involve several complications.[8,9] Homeopathic medicines are quite effective for treating such conditions, as the treatment is based on individualisation. Appropriate selection of similimum and proper dosage often brings about a cure without any complications.[10] According to the World Health Organization, homoeopathy is the second-most widely used system of alternative medicine in healthcare systems worldwide.[11]
Testosterone is believed to play a major role; patients with BPH are found to have low serum testosterone levels. [12,13] Oestrogen may also play a role.[14] BPH may also have a genetic component.[15] Research suggests that the presence of diabetes can affect BPH, as high insulin levels can trigger prostate growth.[16]
Several studies are available that corroborate the efficacy of homoeopathy in treating BPH. Hati et al.’s clinical trial studied 220 men aged 30–90 years with BPH. Patients received constitutional medicines, organopathic medicines or both. Treatment response was the highest in patients who received constitutional and organopathic medicines, although the relief was primarily symptomatic and prostate size remained unchanged.[17] Gupta et al. treated 30 men with BPH and followed up for 1 year. Marked amelioration of symptoms and reduction in prostate size was seen.[18] A case report by Hakma et al. reports a significant reduction in prostate size and residual urine volume with homoeopathic treatment.[19] Manchanda et al. conducted an open, randomised, multicentric, placebo, controlled and clinical trial on 254 patients that reported significant results with the use of organopathic and constitutional remedies in CM potencies.[20] Dole et al. conducted a clinical trial in Pune, Maharashtra from July 2007 to January 2012, in which significant results were found in patients treated with constitutional homoeopathic remedies.[21] Prasad et al. reported a case from their outpatient department (OPD) clinical research unit where BPH treated with Pulsatilla yielded significant improvement.[22] Sharma et al. reported a case from the OPD of Jayoti Vidyapeeth women’s University, where a single dose of Pulsatilla 1M yielded significant relief in a case of BPH.[23] Finally, Oberoi et al. reported a multicentric and observational study of 187 patients, where the most useful medicines were Thuja, Sulphur, Pulsatilla and Lycopodium.[24]
CASE SERIES
Study design
Observational study.
Study setting
This study was conducted at the outpatient department of Mahesh Bhattacharyya Homoeopathic Medical College and Hospital.
Consent
The consents of the patients were obtained.
Inclusion criteria
The following criteria were included in the study:
Male patients above 45 years.
Symptoms of BPH for at least 6 months.
Daytime or nocturnal urinary frequency and urgency.
Difficulty in starting the urinary stream.
Feeling of incomplete urination.
Has not had a previous episode of acute urinary retention.
Has not had previous prostate surgery.
Exclusion criteria
The following criteria were excluded from the study:
Diagnosed with any malignancy of the prostate.
Complete retention of urine for more than 24 h.
Case of urethral stricture.
Having systemic or neurological disorders.
Immunocompromised patients.
Case report 1
A 46-year-old male of moderate socioeconomic status reported to the surgery OPD of Mahesh Bhattacharyya Homoeopathic Medical College and Hospital (MBHMC&H) with a complaint of frequent urge to pass urine at night for 3 months. He had been diagnosed with BPH and was under allopathic treatment. The ultrasonography report showed a prostate gland weighing 29.4 g with dimensions 4.2 × 3.2 × 4.0 cm [Figure 1]. The other investigations such as prostate-specific antigen (PSA) and routine blood investigations were within normal limits. He was advised surgery, but he was unwilling because of the potential complications such as urethral stricture, erectile dysfunction and urinary incontinence. He, therefore, reported to MBHMC&H for homoeopathic treatment.
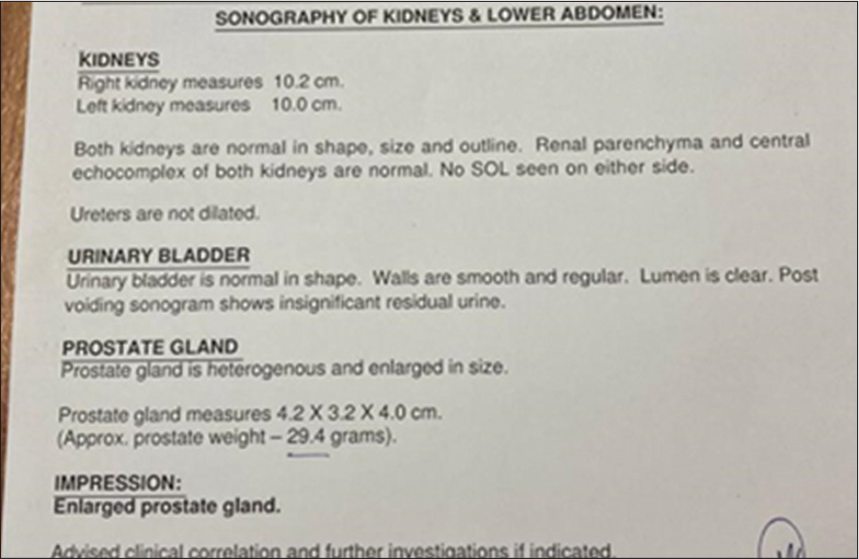
- Ultrasonography of the whole abdomen before the treatment.
Patient information
The patient was very polite and well mannered. He was dressed very soberly and sat upright. His wife complained that he was very obstinate and irritable. He had an extreme craving for sweet things and refused to have any food that had become cold. His thermal reaction was chilly (prefers warm weather). He had easy satiety and had gastric discomfort on consuming rich and spicy food. His bowel movements were unsatisfactory; he passed hard stool every morning. His perspiration was profuse, offensive (especially on the feet) and non-staining. His sleep was sound and he had no particular dreams.
His medical history included dengue fever at age 30 and surgery cholelithiasis 5 years before.
Regarding family history, his father is diabetic and had undergone surgery for BPH at the age of 60. His mother died of a cerebrovascular accident. His maternal uncle has hypertension. After detailed case taking and analysis, the symptoms were evaluated to construct the totality and repertorisation was done. The following characteristic mental general symptoms, as well as physical general and particular symptoms, were considered for repertorisation [Figure 2].[25]
![Repertorisation table. [25]](/content/112/2022/5/4/img/JISH-5-099-g002.png)
- Repertorisation table. [25]
Totality
Obstinate
Irritable
Thermal reaction is chilly
Easy satiety
Desire for sweet foods
Aversion to cold food
Intolerance of rich and spicy food
Stool hard and passed every morning but unsatisfactory
Perspiration is offensive, profuse and more on soles
Frequent urging for urination more at night
After repertorisation and Materia Medica differentiation, Lycopodium was selected as the remedy. Lycopodium 200C (two doses in sac lac for 2 consecutive days to be taken early morning on an empty stomach) followed by placebo (14 doses in globule number 20 and four globules to be taken every night after dinner) was prescribed on 3 December 2020 [Table 1].
| Date | Indication | IPSS Score | Prescription |
|---|---|---|---|
| 3 December 2020 | Frequency of urination at night, extreme chilliness, craving for sweet and irritable | 21 | Lycopodium 200C/2 doses. Daily early morning on an empty stomach for 2 days, followed by placebo for 14 days. |
| 17 December 2020 | Frequency of urination still persists with heaviness; no other complaints. | 18 | Placebo for another 7 days. |
| 24 December 2020 | Frequency of urination is slightly better than before but not satisfactory. No other new complaint. Offensiveness of perspiration reduced considerably. | 16 | Placebo for another 7 days. |
| 31 December 2020 | Urine frequency is much better and passed urine only once at night as detailed by the patient. Advised for whole abdomen ultrasonography to assess the prostate size | 10 | Placebo for another 7 days. |
| 5 January 2021 | Patient doing very well, and the frequency of urination is more than 90% better. Ultrasonography report shows reduced size of the prostate, weight 15 g [Figure 3]. | 6 | Placebo for another 30 days. |
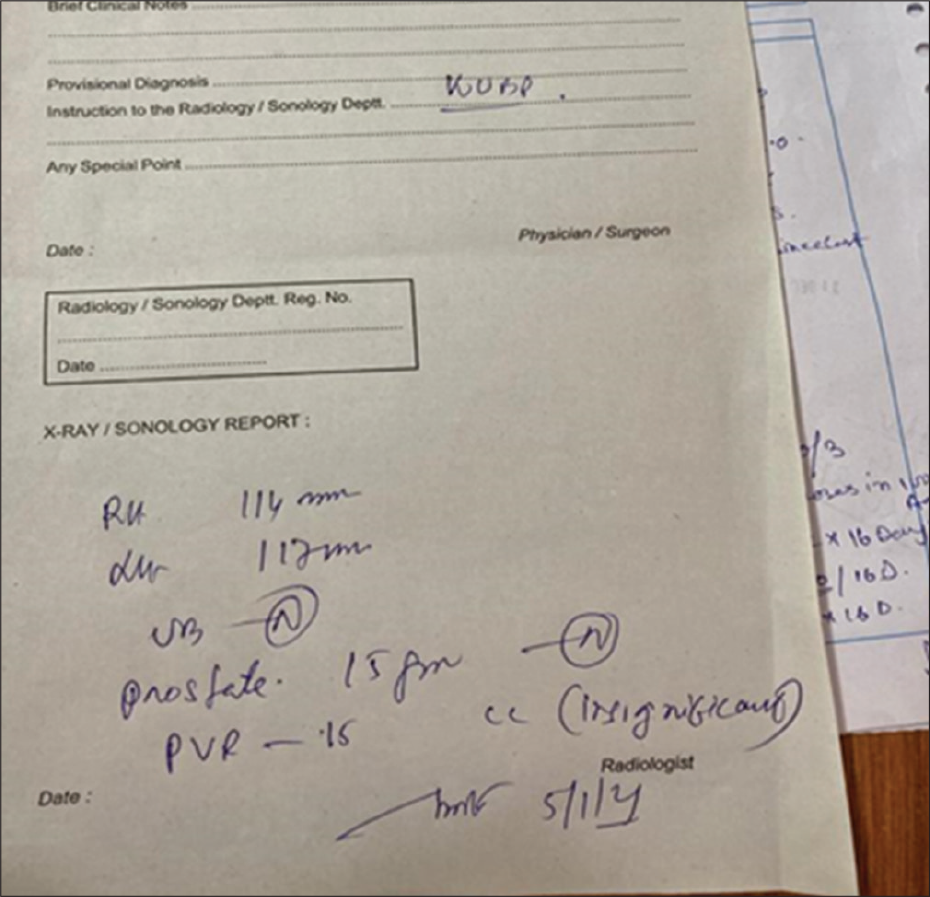
- Ultrasonography of the whole abdomen after the treatment.
Case report 2
A 52-year-old male of poor socioeconomic status visited the surgery OPD of MBHMC&H with a complaint of frequent urge to pass urine at night for the past 6 months.
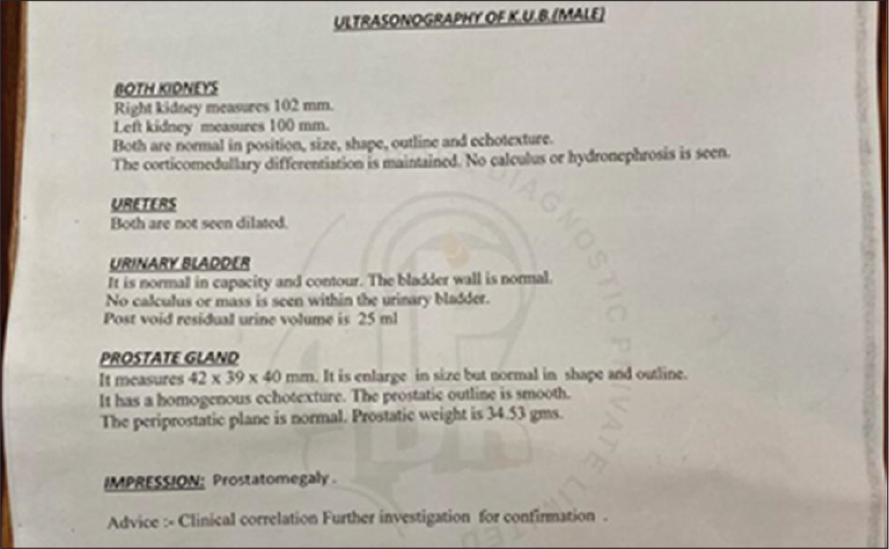
He had been diagnosed with BPH and did not want to undergo surgery. On USG, the prostate gland weighed 77 g and dimensions were 35 × 37 × 44 mm [Figure 4]. The PSA and routine blood test results were within normal limits.
- Ultrasonography of the whole abdomen before the treatment.
Patient information
The patient was mild-mannered but kept saying he had no problem. He had an extreme craving for sweet things and cold things. His thermal reaction is chilly (prefers warm weather). His appetite is adequate and he prefers green vegetables rather than fish and meat. His bowel movements were irregular and he frequently had morning diarrhoea. His perspiration was offensive (especially in the genital area), profuse and non-staining. He had multiple warts all over his body. His sleep was sound and he had no particular dreams. His medical history included typhoid fever at the age of 25 years. His father and paternal grandfather had bronchial asthma as well. He works as a labourer in an iron goods manufacturing company. On detailed case taking and analysis, the symptoms were evaluated to construct the totality and repertorisation was done.
The characteristic mental general symptoms, as well as physical general and particular symptoms, were considered for repertorisation [Figure 5].[25]
![Repertorisation table.[25]](/content/112/2022/5/4/img/JISH-5-099-g005.png)
- Repertorisation table.[25]
Totality
Mild natured
Refused to accept the fact that he had complaints
Thermal reaction is chilly
Desire for green vegetables, sweets and cold food
Stool is irregular; frequent morning diarrhoea
Offensive and profuse perspiration of the genitals
Multiple warts all over his body
Frequent urge to pass urine at night
After repertorisation and Materia Medica differentiation, Thuja occidentalis was selected as a remedy. T. occidentalis 30C (two doses in sac lac for 2 consecutive days to be taken early morning on an empty stomach) followed by placebo (14 doses in globule number 20 and four globules to be taken every night after dinner) was prescribed on 24 October 2019 [Table 2].
| Date | Indication | IPSS Score | Prescription |
|---|---|---|---|
| 24 October 2019 | Frequency of urination at night, extreme chilly, desire for cold food, morning diarrhoea and offensive perspiration of genitalia | 23 | Thuja occidentalis 30C/2 doses. Daily early morning on empty stomach for 2 days, followed by placebo for 14 days. |
| 7 November 2019 | Frequency of urination same. | 21 | Placebo for another 14 days. |
| 21 November 2019 | Frequency of urination was slightly reduced no other new complaints. Medicine was not repeated as the patient was improving | 15 | Placebo for another 21 days. |
| 12 December 2019 | Urine frequency is much better and passed urine once at night as detailed by the patient. Diarrhoea in the morning is improved. No other complaints. |
12 | Placebo for another 21 days |
| 2 January 2020 | The patient doing very well, and the frequency of urination is more than 90% reduced. The patient advised ultrasonography of KUB and prostate. | 10 | Placebo for another 21 days. |
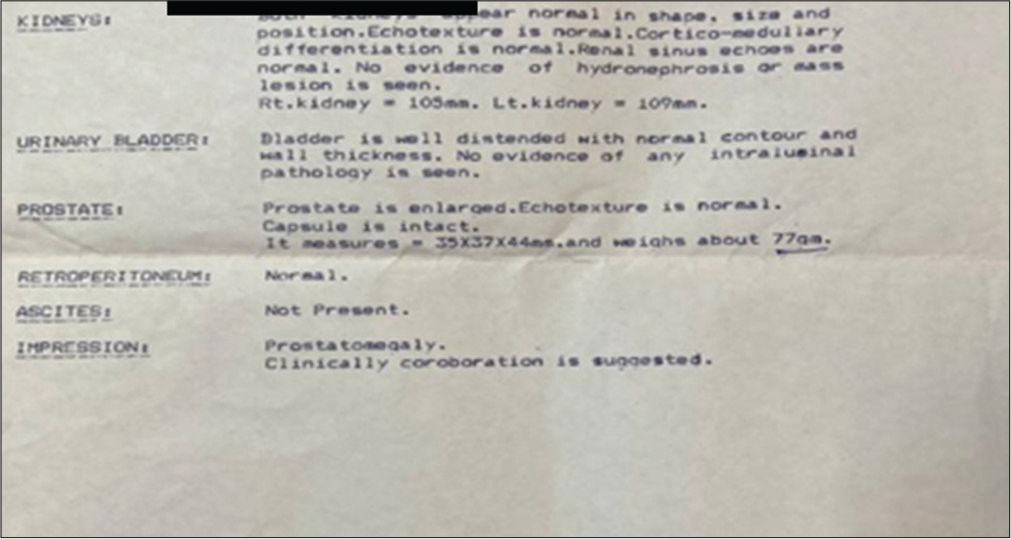
| 13 February 2020 | No previous symptoms. Improved clinical and subjective symptoms. The ultrasonography report (8 February 2020) showed a prostate weighing 34.53 g [Figure 6]. |
8 | Placebo for another 30 days. |
- Ultrasonography of whole abdomen after the treatment.
The patient stopped following up as he was better.
Case report 3
A 68-year-old male with poor socio-economic status visited the surgery OPD of MBHMC&H complaining of incontinence of urine with an unfinished sensation and increased nocturnal frequency for 4 months.
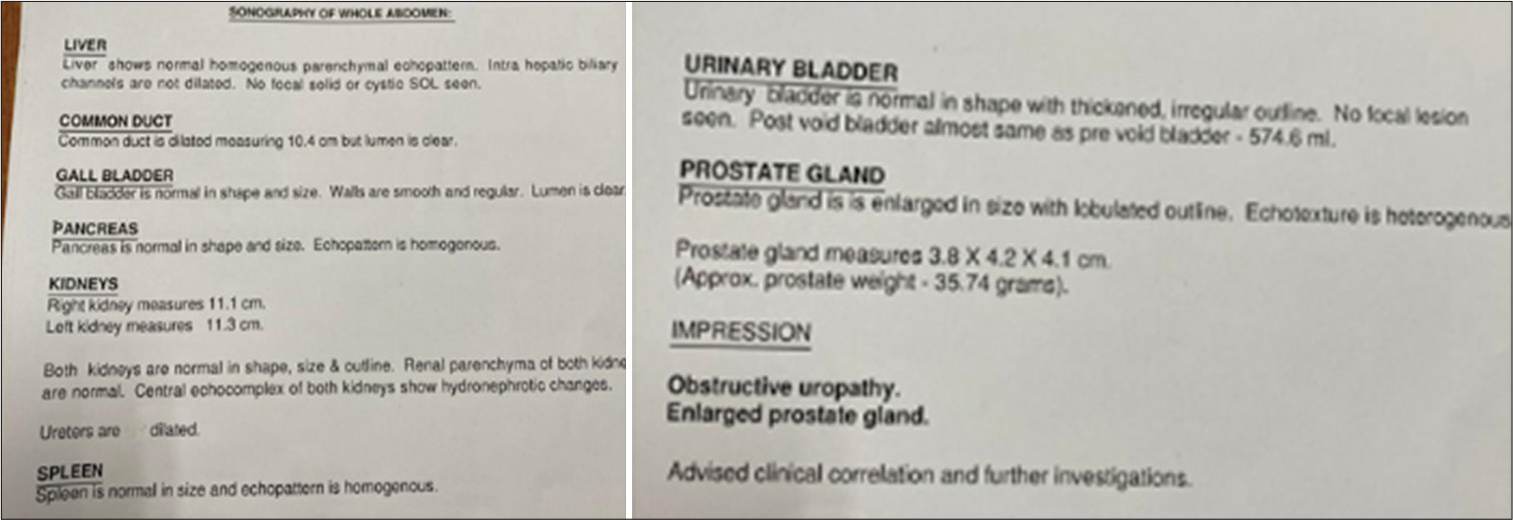
On USG, the prostate gland weighed 79 g. The PSA level was 7.6 ng/mL and the acid phosphatase level was 7.12 u/L [Figure 7].
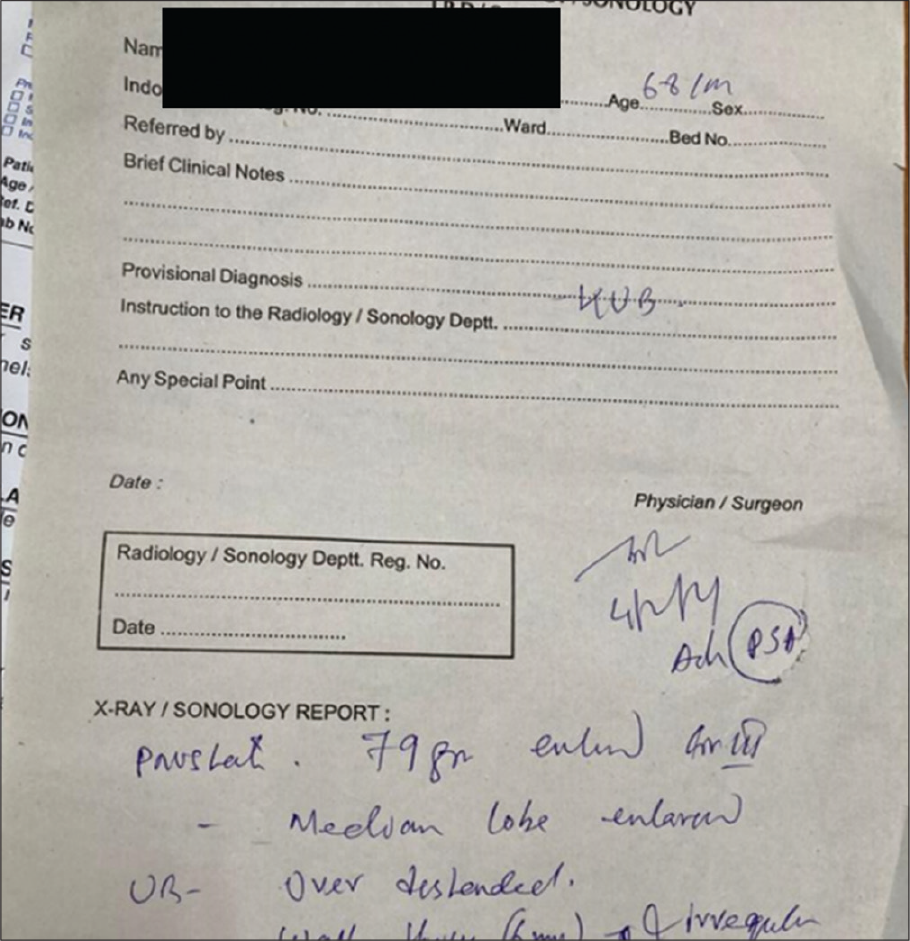
- Ultrasonography of the whole abdomen before the treatment.
Patient information
The patient was very fastidious. He was very anxious about his condition. He had an extreme craving for sweets and refused to have any food that had become cold. His thermal reaction is chilly and he feels better during the summer season. His appetite is adequate and he craves raw onion, fish, tea and sour foods. His bowel movements were regular but unsatisfactory. His medical history included pulmonary tuberculosis at the age of 27, treated with DOTS. His family history included: Mother: Asthma and father: Diabetes and osteoarthritis. On detailed case taking and analysis, the symptoms were evaluated to construct the totality and repertorisation was done. The characteristic mental general symptoms, as well as physical general and particular symptoms, were considered for repertorisation [Figure 8].[25]
![Repertorisation table.[25]](/content/112/2022/5/4/img/JISH-5-099-g008.png)
- Repertorisation table.[25]
Totality
Anxious
Thermal reaction is chilly
Desire for sweets, raw onion, fish, tea and sour foods
Aversion to cold food
Stool is regular but unsatisfactory
History of pulmonary tuberculosis
Incontinence of urine
Frequency of micturition at night
After repertorisation and Materia Medica differentiation, Arsenic album was selected as a remedy. A. album 200 C (two doses in sac lac for 2 consecutive days to be taken in the early morning on empty stomach) followed by a placebo (14 doses in globule number 20 and four globules to be taken every night after dinner) was prescribed on 4 February 2021 [Table 3].
| Date | Indication | IPSS Score | Prescription |
|---|---|---|---|
| 4 February 2021 | Frequency of urination at night, extreme chilly, desire for raw onion, tea-drinking habit and fastidious. Anxious about his complaints. | 30 | Arsenic album 200C/2 doses. Two days early morning on empty stomach for 2 days, followed by placebo for 14 days. |
| 18 February 2021 | Frequency of urination still persists. | 30 | Placebo for another 14 days. |
| 4 March 2021 | The frequency of urination is slightly better than before, with no other new complaint. Anxiety is no more present. | 25 | Placebo for another 14 days. |
| 18 March 2021 | Urine frequency is much better and passed urine once at night as detailed by the patient. No other complaints. | 9 | Placebo for another 21 days. |
| Loss to follow-up | After that, the patient stopped attending the OPD. His subjective symptoms were much reduced during his past follow-up. The BOO was significant in the reports [Figure 7] and the post-void urine was also much increased. In spite of the pathology still existing, the complaints were significantly lessened and prostate size was also reduced [Figure 9]. No pathology could be found for this yet and more clinical investigations such as urethral ultrasound, and uroflowmetry were advised to find out the pathology behind increased post-void residual urine. |
IPSS: International Prostate Symptom Score
DISCUSSION
In cases of BPH, determining the clinical symptoms and a thorough investigation into the patient’s personal, medical and family history enables a physician to determine the correct remedy and treatment plan. Homoeopathic management through proper individualisation and proper case taking can make a significant difference in the treatment of BPH. The previous observational and experimental studies have shown that individualised homoeopathic treatment has been very successful in cases of BPH,[18-21] along with mother tinctures and other measures. This is an observational study and results were obtained with clinical and pathological improvements in the patients [Figures 3, 6, 9]. The cases were prescribed the indicated remedies based on individualisation. The primary limitation of this study was that the study population is only three patients. Randomised controlled trials and/or observational studies with larger sample sizes are needed to collect more detailed information.
- Ultrasonography of the whole abdomen after the treatment.
CONCLUSION
The above-discussed cases show that homoeopathic medicines, when selected using the process of individualization, can bring about improvements in symptoms and clinical signs. Homoeopathy teaches us to treat not the disease but the patient as a whole. We hope that these cases will provide positive examples for homoeopaths and help them to treat such cases with confidence.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Bailey and Loves Short Practice of Surgery (26th ed). United States: CRC Press; 2018. p. :1341-2.
- [Google Scholar]
- Harrison's Manual of Medicine (18th ed). Ch. 81. United States: McGraw Hill Publication; 2019. p. :469-70.
- [Google Scholar]
- Kumar and Clark's Clinical Medicine (17th ed). New York: Saunders Elsevier Ltd; 2009. p. :645.
- [Google Scholar]
- What do we really know about benign prostatic hyperplasia and lower urinary tract symptoms in adult men? World J Urol. 2011;29:141-2.
- [CrossRef] [PubMed] [Google Scholar]
- Urologic diseases in America project: Benign prostatic hyperplasia. J Urol. 2005;173:1256.
- [CrossRef] [PubMed] [Google Scholar]
- The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349:2387-98.
- [CrossRef] [PubMed] [Google Scholar]
- The economics of benign prostatic hyperplasia treatment: A literature review. Clin Ther. 1996;18:1227-41.
- [CrossRef] [PubMed] [Google Scholar]
- Mortality and reoperation after open and transurethral resection of the prostate for benign prostatic hyperplasia. N Engl J Med. 1989;320:1120-24.
- [CrossRef] [PubMed] [Google Scholar]
- Mortality, morbidity and complications following transurethral resection of the prostate for benign prostatic hypertrophy. J Urol. 1992;147:1566-73.
- [CrossRef] [PubMed] [Google Scholar]
- Homoeopathy In: Jonas WB. Levin JS, editors. Essentials of Complementary Medicine. United States: Lipincott Williams Wilkins; 1999.
- [Google Scholar]
- Serum steroids in relation to benign prostatic hyperplasia. Oncology. 1997;54:497-501.
- [CrossRef] [PubMed] [Google Scholar]
- Serum sex hormones and measures of benign prostatic hyperplasia. Prostate. 2004;61:124-31.
- [CrossRef] [PubMed] [Google Scholar]
- Oestrogen and benign prostatic hyperplasia: Effects on stromal cell proliferation and local formation from androgen. J Endocrinol. 2008;197:483-91.
- [CrossRef] [PubMed] [Google Scholar]
- Genetic determinants of metabolism and benign prostate enlargement: Associations with prostate volume. PLoS One. 2015;10:e0132028.
- [CrossRef] [PubMed] [Google Scholar]
- Hyperglycemia and insulin resistance and the risk of BPH/LUTS: an update of recent literature. Curr Urol Rep. 2014;15:462.
- [CrossRef] [PubMed] [Google Scholar]
- Constitutional, organopathic and combined homeopathic treatment of benign prostatic hypertrophy: A clinical trial. Homoeopathy. 2012;101:217-23.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical evaluation of homoeopathic medicines in benign prostatic hyperplasia. Homoeopathic Links. 2019;32:82-7.
- [CrossRef] [Google Scholar]
- Benign prostatic hyperplasia: An evidence-based case report treated with Homoeopathy. Indian J Res Homoeopathy. 2018;12:101-6.
- [CrossRef] [Google Scholar]
- Proceedings of the XXX GIRI meeting; 2016 Sep 09-11; Netherland. Int J High Dilution Res. 2016;15:12-3.
- [Google Scholar]
- The health outcome after Homoeopathic treatment in case of BOH and LUTS: A prospective clinical study. Journal of Pharmaceutical and Biomedical Sciences. 2012;22:1-7.
- [Google Scholar]
- Benign prostatic hyperplasia and its Homoeopathic approach. Global J Fir Res Anal. 2020;9:36106.
- [Google Scholar]
- Treatment of benign prostatic hyperplasia in Homoeopathy with repertorial analysis-a case study. Eur J Mol Clin Med. 2020;7:1260-77.
- [Google Scholar]
- Homoeopathic medicines in the management of benign prostatic hyperplasia: A multi-centric prospective observational study. IJRH. 2019;12:113-124.
- [CrossRef] [Google Scholar]
- Hompath Zomeo 3.0 Software, using Kent's Repertory Mind Technologies Pvt. Ltd. Mumbai, Maharashtra, India: Mind Technologies; 2002.
- [Google Scholar]




