
Translate this page into:
Management of Stage 3 Haemorrhoids with Homoeopathy – A case report
*Corresponding author: Dr. Dhanya Deepak Bhat, Department of Practice of Medicine, A. M. Shaikh Homoeopathic Medical College, Hospital and PG Research Centre, Belagavi 590010, Karnataka, India. dhanyadbhat23@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Vijaykumar J, Bhat DD. Management of Stage 3 Haemorrhoids with Homoeopathy – A case report. J Intgr Stand Homoeopathy 2022;5:107-11.
Abstract
Haemorrhoids are abnormal masses of dilated blood vessels that can occur both internally and externally in the rectum. This is a case report of a 60-year-old woman who presented with complaints indicating Stage 3 haemorrhoids with a longstanding history of constipation. After acute case taking, observing the pathological progress of the disease and repertorising, Aesculus hippocastanum was prescribed. The patient’s condition and improvement were evaluated using the bleeding, prolapse, reduction, skin tags and thrombosis classification and staging at each follow-up. The patient showed marked improvement within a month. This case report emphasises the role of homoeopathic medicines in cases of haemorrhoids.
Keywords
Haemorrhoids
Bleeding
prolapse
thrombosis
Aesculus hippocastanum
Homoeopathy

INTRODUCTION
Haemorrhoids or piles are defined as distal displacement and enlargement of the normal anal cushion. Haemorrhoids are the fourth leading outpatient gastrointestinal diagnosis, affecting men and women equally as per global prevalence.[1]
Haemorrhoids are classified based on their location and degree of prolapse.
Internal haemorrhoids originate from the inferior haemorrhoidal venous plexus above the dentate line and are covered by mucosa. External haemorrhoids are dilated venous plexus located below the dentate line, covered with squamous epithelium and innervated by cutaneous nerves, which are branches of the pudendal nerve.[2] Lunniss et al. state that external haemorrhoids are not a separate anatomical entity, but an extension of internal haemorrhoids, representing an evolutionary complication.[3]
A 2018 study from Bangalore, Karnataka stated that the prevalence is higher in those aged 30– 60 years and rare in those under 20 years.[4,5] Multiple factors are responsible for the development of haemorrhoids, including a history of constipation and prolonged straining while defecation.[2]
Diagnostic assessment of haemorrhoids is usually done with the Goligher classification; however, it was deemed inadequate as it does not consider the associated symptomatology and extension of classification to the entire haemorrhoidal system is not available.[3] Júnior et al. presented a new classification for haemorrhoidal disease, the bleeding, prolapse, reducibility, skin tags and thrombosis (BPRST) classification, which overcomes the limitations of the Goligher classification.[6] Each element of the BPRST classification is further numbered to obtain a more precise diagnosis of an individual patient’s state.
Details are shown in [Table 1].
| Bleeding (B) | Prolapse (P) | Reduction (R) | Skin tags (S) | Thrombosis (T) |
|---|---|---|---|---|
| B0–No Bleeding | P0–No prolapse | R0–spontaneous reduction | S0–No skin tags | T0–Without acute Thrombosis |
| B1–Bleeding | P1–Prolapse of 1 pile | R1–Manual reduction | S1–Symptomatic skin tags | T1–With thrombosis |
| - | P2–Prolapse of 2 or more piles | R2–Irreducible prolapse | - | - |
| Clinical staging | Bprst description | Indication | ||
| Stage 1 | B1, P0, R0, S0, T0 | Patients with bleeding, with no report of prolapse and external components, that is, skin tags or thrombosed piles | ||
| Stage 2 | Any B, P1/P2, R0/R1, T0 | Patients with prolapse (regardless of the number of piles) that can be reduced spontaneously or by digital manoeuvre | ||
| Stage 3 | Any B, P1/P2, R2, S1, T1 | Patients with irreducible prolapse, symptomatic skin tags with acute haemorrhoidal thrombosis | ||
Conservative treatment includes lifestyle and dietary changes with topical treatment such as hydrocortisone cream and anti-itch medications. Non-surgical procedures include rubber band ligation, sclerotherapy and infrared coagulation. However, these may cause complications including pain, urinary retention, discomfort, bleeding and (very rarely) perineal sepsis. If symptoms persist despite conservative treatment, surgery is suggested.
In many cases, prescription of homoeopathic medicines is possible, where medicine is selected based on the similarity to the disease process or pathological changes at the tissue level.[7] Such a course of treatment may help prevent surgery. A study has shown the effectiveness of homoeopathic medicines in treating haemorrhoid cases.[8] Here, we present a case of external haemorrhoids treated with the homoeopathic remedy Aesculus hippocastanum.
CASE REPORT
A 60-year-old married woman, housewife, with an average height and moderate build visited the outpatient department of A.M. Shaikh Homoeopathic Medical College and Hospital on 29 November 2021.
Presenting complaints with details
The presenting complaints are described below [Table 2].[9]
| Location | Sensation | Modalities | Concomitants |
|---|---|---|---|
| Rectum Onset–Sudden Duration–1 week |
Stitching type of pain++ in the anal region Intolerable pain No discharge or bleeding |
Aggravated while walking+ and sitting Amelioration–none |
None |
| Anus Onset–Sudden Duration–1 week |
Sensation as if the mass is protruding and blocking the anal canal | Aggravated while walking+ and sitting Amelioration–none |
None |
Medical history
She has osteoarthritis from 8 years, Diabetes Mellitus and Hypertension from last 4 years, on conventional and homoeopathic treatment since diagnosis.
Physical generals
She is fair, moderately built and nourished with a good appetite, but irregular in her diet/eating patterns. She has a history of intermittent fasting on and off. Her bowels are constipated, with difficulty in evacuating stools. She is a chilly patient.
Examination findings
General
Temperature – afebrile. Pulse – 80 beats/min. Respiratory rate: 17 cycles/min. Blood pressure – 130/90 mmHg. No pallor.
Systemic
Respiratory system – Air entry bilaterally equal. Cardiovascular system – S1 and S2 heard. Per abdomen – no abnormality detected. Central nervous system – conscious and oriented.
Local examination
On inspection, there was a protrusion of a mass, possibly two with swelling around the anal orifice and blue in colour. No discharge/bleeding from the affected site [Figure 1].

- First visit, 29 November 2021.
A digital examination was not done as she reported intense pain and tenderness.
Diagnostic assessment
Complaints of the patient and local rectal examination suggested a diagnosis of external haemorrhoids. The BPRST classification was used to evaluate and grade the most frequent complaints.
Totality of symptoms
Mass protruding from the anal canal without bleeding or discharge
Mass protruding from the anal canal is bluish in colour
Sensation as if a mass is protruding and blocking the anal canal
Stitching type of pain in the anal region
Aggravation from walking and sitting
Constipated stools were difficult to evacuate.
Repertorial totality
Rectum – Haemorrhoids – External
Rectum – Haemorrhoids – Protruding – Prolapsed
Rectum – Haemorrhoids – Bluish
Rectum – Haemorrhoids – blind
Rectum – Pain – stitching, sharp
Rectum – Haemorrhoids – Walking – Aggravation
Rectum – Haemorrhoids – Sitting – Aggravation
Rectum – Constipation – Difficult stool.
Repertorial analysis was done with complete repertory using Hompath classic version 8.0 [Figure 2].
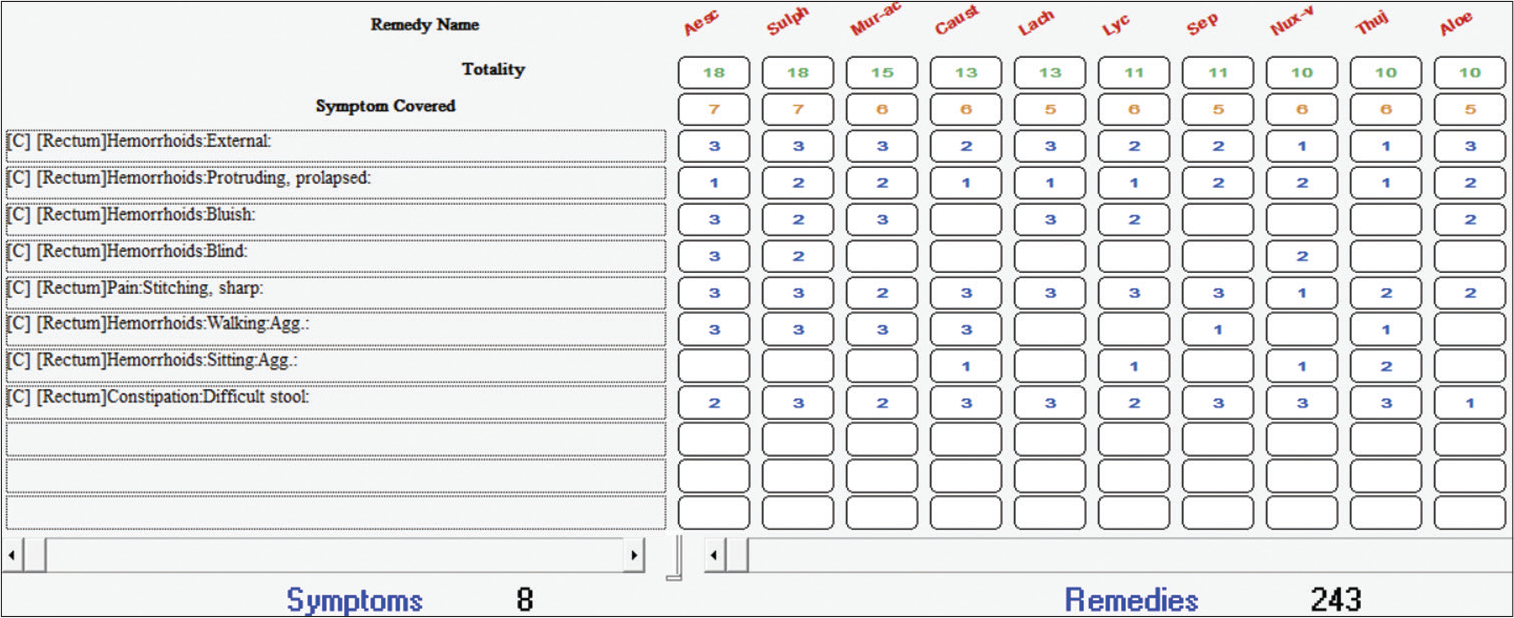
- Repertorial sheet using hompath classic software, Mind Technologies, Mumbai, India.
Therapeutic intervention
After acute case taking and repertorial analysis, A. hippocastanum, Sulphur and Muriaticum acidum were found to cover the symptoms of the patient. The patient did not complain about itching and burning, which is marked in Sulphur; therefore, Sulphur was ruled out. Muriaticum acidum is mostly indicated in involuntary evacuation of faeces while urinating along with itching and bleeding haemorrhoids, which were not seen in the patient. Finally, after thorough Materia Medica differentiation[10] A. hippocastanum was prescribed as a pathological prescription considering its action on the rectal veins; the haemorrhoidal vessels become intensely congested. This leads to violent inflammation of the anus and rectum, producing haemorrhoids in their most aggravated form. Aesculus also covers most of the symptoms like large blue-coloured haemorrhoids which block up the rectum, with sharp stitching pain in the anus, and no tendency to bleed, all of which were seen in our patient.[11,12]
In general, low and moderate potencies in repeated doses are effective for advanced pathological conditions.[7] Accordingly, in this case, 30C potency was prescribed for a day with three doses.
Follow-ups and outcomes
Changeability in symptoms, BPRST classification and staging were done at every follow-up. Details are shown in [Table 3].
| S. No. | Date of visit | Symptoms | BPRST Classification | Prescription |
|---|---|---|---|---|
| 1 | First visit 29 November 2021 |
Intolerable stitching type of pain and tenderness in the anal region with feeling as if some mass is protruding and blocking the anal canal, aggravated by walking and sitting with constipation for a long time | B0, P2, R2, S1, T1. Stage 3 [Figure 3] |
Aesculus hippocastanum 30C Thrice a day |
| 2 | 30 November 2021 2nd day |
After two doses of medicine, pain had reduced to 50%, but immediately after taking third dose of medicine, pain aggravated a bit. Bowels were satisfactory. No any new complaints were noted | B0, P2, R2, S1, T1 Stage 3 |
Placebo 30/2 days/Thrice a day. The patient was asked to report after 2 days |
| 3 | 1 December 2021 4th day |
Pain in anal region still persists. No new complaints were noted | B0, P2, R2, S1, T1 Stage 3 |
Aesculus hippocastanum 30C/3 doses/thrice a day. Instructed her to stop the medicine immediately once the pain is better |
| 4 | 10 December 2021 | After taking one dose of medicine, Pain and tenderness in rectum is reduced. Feeling of protrusion of mass from anal canal only during passing stools and spontaneously reduced after passing stools. Bowels: clear and satisfactory On inspection: Swelling around anal canal is reduced. The mass protrudes only on straining and spontaneously reduces |
B0, P1, R0, T0 Stage 2 [Figure 3] |
Placebo/thrice a day/1 month |
| 5. | 18 January 2022 | All complaints recovered. No new complaints were noted | B0, P0, S0, T0 [Figure 4] |
Placebo/1 week/Thrice a day |

- 10 December 2021.

- 18 January 2022.
DISCUSSION
External haemorrhoids are always considered to be effectively managed with surgery. However, in this case, the patient opted for homoeopathic treatment. Consideration of the patient’s most peculiar presenting symptoms and pathological changes indicated A. hippocastanum. A study by Ezberci et al. highlighted on the effectiveness of A. hippocastanum in the treatment of every stage of haemorrhoids due to its antiseptic, venotonic, vasoprotective and anti-inflammatory properties, which are due to its aescin content.[13]
In this case, after the third visit, the complaints had not improved further; hence, we repeated the same medicine and potency with the instructions to stop the medicine once the pain reduces. Later, a single dose of medicine helped to improve the patient’s complaints subjectively; objectively, changes in the BPRST classification and staging were observed as well.
CONCLUSION
This case experience emphasises the role of homoeopathy in cases of Grade 3 haemorrhoids, preventing surgery. Consideration of pathological phenomena in the evolution of disease helped to select the remedy in this acute case. However, further larger studies with large sample sizes are required to assess the efficacy of homoeopathic treatment in Stage 3 haemorrhoids.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Review of hemorrhoid disease: Presentation and management. Clin Colon Rectal Surg. 2016;29:22-9.
- [CrossRef] [PubMed] [Google Scholar]
- Hemorrhoids: From basic pathophysiology to clinical management. World J Gastroenterol. 2012;18:2009-17.
- [CrossRef] [PubMed] [Google Scholar]
- Classification and guidelines of hemorrhoidal disease: Present and future. World J Gastrointest Surg. 2019;11:117-21.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of hemorrhoid among the patients visiting surgery OPD at NIUM hospital. Eur J Biomed. 2018;5:435-7.
- [Google Scholar]
- A new classification for hemorrhoidal disease: The creation of the “BPRST” staging and its application in clinical practice. Ann Coloproctol. 2020;36:249-55.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://www.nhp.gov.in/principles-ofprescribing_mtl [Last accessed on 2022 Mar 15]
- Prospective clinical study of hemorrhoids with individualized homeopathic treatment. J Med Sci Clin Res. 2018;6:372-8.
- [CrossRef] [Google Scholar]
- Boenninghausen's Characteristics Materia Medica and Repertory with Word Index Uttar Pradesh: B Jain Publishers; 2021.
- [Google Scholar]
- A Dictionary of Practical Materia Medica New Delhi, India: B Jain Publishers; 1995.
- [Google Scholar]
- A Synoptic Key to the Materia Medica: (A Treatise for Homoeopathic Students) New Delhi: B Jain Publishers; 1996.
- [Google Scholar]
- Physiological Materia Medica, Containing all that is Known of the Physiological Action of our Remedies: Together with their Characteristic Indications and Pharmacology Chicago: Gross and Delbridge; 1881.
- [Google Scholar]
- Aesculus hippocastanum (aescin, horse chestnut) in the management of hemorrhoidal disease: Review. Turk J Colorectal Dis. 2018;28:54-7.
- [CrossRef] [Google Scholar]




