
Translate this page into:
Homoeopathy for alcohol withdrawal state with delirium – A case report
*Corresponding author: Dr. S. Karunakara Moorthi, Research Officer(H), Department of Psychiatry, National Homoeopathy Research Institute in Mental Health, Kottayam, Kerala, India. dr.karunakaramoorthi@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Karunakara Moorthi S. Homoeopathy for alcohol withdrawal state with delirium – A case report. J Intgr Stand Homoeopathy. 2024;7:192-6. doi: 10.25259/JISH_82_2023
Abstract
Alcohol withdrawal syndrome’s major consequence, delirium tremens, is a complex issue that greatly raises patient morbidity and fatality rates. Alcohol withdrawal delirium is characterised by tremors, hypertension, profuse sweating, tachycardia and common delirium symptoms such as disorientation, lightheadedness, disturbances of circadian rhythm, processes of thinking and sensory disorders, all occurring over time. A 54-year-old male patient presented with a feature of visual hallucination that the police were standing in front of his house. He had suspicion that someone had kept a listening device in his house and all his conversations were being heard. He was doubtful that he could hear a musical tone and constantly searched for the music-producing device in his clothes, on his body, in his house, etc. As per his acute symptoms presentation, Arsenicum album (Ars. alb) 30 C was prescribed frequently until his symptoms responded to it. His symptoms completely disappeared, and his Clinical Institute Withdrawal Assessment for Alcohol score decreased from 16 to 0 within 5 days. This case report illustrates the potential use of homoeopathic medicine in the management of an acute emergency of Alcohol Withdrawal Delirium.
Keywords
Alcohol withdrawal delirium
Arsenicum album
Clinical institute withdrawal assessment for alcohol
Homoeopathy

INTRODUCTION
Alcohol withdrawal symptoms range from mild symptoms such as insomnia and tremors to severe complications such as withdrawal seizures and delirium tremens (DTs). Alcohol withdrawal syndrome appears after a significant reduction or complete discontinuation of alcohol consumption in patients with alcohol dependence.[1] The prodromal symptoms typically include insomnia, tremulousness and fear. Withdrawal convulsions may also precede the onset. The classical triad of symptoms consists of clouding of consciousness and confusion, vivid hallucinations and illusions affecting any sensory modality and pronounced tremors. Delusions, agitation, insomnia and restlessness are also usually present.[2] Tremors develop within 6–8 hours of stoppage of drinking. Psychiatric and cognitive symptoms begin at 8–12 hours, seizures begin at 12–24 hours, and DTs occur at any time during the first 72 hours. Delirium is an acute clinical emergency with psychiatric symptoms and signs that happen in quite a few settings and is more unusual in places such as intensive care units (ICUs) and palliative care facilities. People with delirium pose a danger to themselves and others because of their unpredictable behaviour. People with delirium may become aggressive, have suicidal thoughts and react to hallucinations and delusional thoughts as if they were real dangers.[3] The prevalence and incidence of delirium in various ICUs in India have reportedly ranged from 16.1–68.2% to 8–59.6%, respectively. Methodological discrepancies exist between research. Depending on the study context, different non-ICU settings have different prevalence rates. According to data from India, the death rate for delirium patients admitted as inpatients ranges from 6.7% to 30.7%.[4] It is now well established that people with chronic alcohol abuse develop this symptom within 48 hours after abruptly quitting alcohol. Without proper treatment, the mortality rate is expected to be as high as 37%. Long-term alcohol exposure reduces gamma-aminobutyric acid (GABA) activity over time, altering the type and function of GABA receptors. Abrupt cessation of alcohol consumption reduces the inhibitory effect of GABA neurotransmitters, causing hyperactivity of the central nervous system. Alcohol also blocks the action of the N-methyl-D-aspartate receptor by acting as a receptor antagonist. Stopping alcohol abruptly increases the action of glutamic acid, resulting in a strong stimulant effect. This may be the reason for the clinical manifestation of sympathetic hyperactivity, such as agitation, tremors, tachycardia and hypertension.[5]
In Homoeopathy, a few studies have been conducted favouring homoeopathic intervention. Milewska, et al. reported a case series of 30 male patients who were prescribed Sulphur 30X and later other homoeopathic medicines.[6] Various studies have highlighted the effectiveness of homoeopathy in managing alcohol withdrawal delirium. Another case series involving 30 male patients who were prescribed Sulphur 30X demonstrated its positive effect on alcoholic delirium tremens, with improvement observed within a short duration.[7] A randomised comparative trial proved that individualised Homoeopathy is not inferior to standard allopathic treatment in the management of alcohol-dependence patients.[8] A retrospective cohort study has shown the significant role of Homoeopathic medicine in the management of acute alcohol withdrawal syndrome.[9]
This study used a short, standardised scale known as the Clinical Institute Withdrawal Assessment for Alcohol (CIWAAr),[10] which consisted of ten questions to assess the severity of alcohol withdrawal syndrome clinically. This scale offers increased efficiency, retaining clinical usefulness, validity and reliability. The total maximum score is 67. The score of (<10) indicates minimal, (10–20) as moderate and (>20) as severe.
To add more evidence on homoeopathic management of alcohol withdrawal delirium, a clinical case report shows significant improvement in the symptoms exclusively with homoeopathic treatment.
CASE REPORT
Patient information
A 54-year-old male patient who worked as a catering supervisor came to the Outpatient Department of a tertiary care hospital in Kottayam, Kerala, on May 20, 2023, along with his wife, complaining that he did not sleep throughout the day and night for the past 4 days, constantly saying that someone was coming to kill him and his wife. He could visualise the police standing in front of his house, but his wife could not. Suspicious that someone was listening to whatever they spoke and kept a recorder at home. He was doubtful that he could hear a musical tone and constantly searched for the music-producing device in his trousers, under the table, on his body, etc.
History of presenting complaint
He has been using alcohol from the age of 32 years. He used to take an average of 300 mL of Rum per day. Before 1 month, his wife was out of the station, and the patient was alone at home. He started drinking alcohol (Rum) at home for the whole day, around 500 mL and the next day, he complained of vomiting, nausea, weakness and reduced appetite with trembling hands after waking up in the morning. He informed his wife of the complaints and she returned immediately. He stopped drinking alcohol immediately the next day, and his complaints were reduced except for the trembling of his hands. On May 15, 2023, the night ahead, he started showing symptoms of restlessness with anger and irritability. He was so restless that he walked across the room constantly. He was constantly telling his wife that people were listening to their talks and would come to kill them. Hence, he was repeating that he would commit suicide to rescue his wife from them. He contemplated suicide to escape from being killed by the people watching them. He had a fear of death, darkness and being alone. He was suspicious that police were standing in front of his home to arrest him, but he did not know the reason, and he was walking to and fro in the room, shouting and saying to the police that he was innocent. He could hear a musical tone and constantly searched for the music-producing device in his pants, under the table, on his body, etc.
Past history
At the age of 46 years, he had oesophageal varices Grade 1, portal hypertensive gastropathy and haemoptysis, so he was admitted to the hospital, took conventional medicine for 2 months and then discontinued.
At the age of 47, he had a very mild suspicious episode after a sudden withdrawal from alcohol, and he was relieved within 2 days without treatment.
Family history
His paternal grandmother suffered from non-insulin-dependent diabetes mellitus. His paternal uncle had a psychiatric illness.
Personal history
The prenatal and postnatal history was uneventful. All the developmental milestones were achieved at the appropriate time. He had taken all the vaccinations at the proper time.
Life space investigation
He was born in a lower-middle-class family as the 4th child (last child). He was in a good relationship with his parents and siblings. He was below average in his studies. His school life was uneventful. He failed his pre-degree. He discontinued the Industrial Training Institute due to difficulty. Henceforth, he started working in Catering, and now, he works as a catering supervisor. He has been consuming alcohol since the age of 32, and he used to take an average of 300 mL of Rum daily. He got married at 34 years old. They did not have children. He had a low sperm count, and his wife had a uterine fibroid. They tried in vitro fertilisation (IVF) but were not successful. He loves his wife so much that whenever she goes to her parent’s house, he always calls her and asks her to return soon. He is in a good relationship with his wife, and they have been fine about their childlessness. In general, he desires company, fears darkness and is anxious about his health. He is fastidious and a workaholic. He never drinks during his working hours.
Physical generals
He had increased thirst and was unsatisfied, so he drank water frequently. He had been sleepless for 4 days. Thermally, he was an ambithermal person.
Clinical findings (Mental status examination baseline)
The mental status examination was done during the first consultation, and the patient was found to be average-kempt, conscious, orientated and aware of his surroundings but confused. He seemed to be suspicious, restless and fearful. He established rapport with the physician with fear and suspicious talk. He maintained eye-to-eye contact. He had Increased Psychomotor Activity. His interpersonal relationships appeared satisfactory. His speech was irrelevant, but Rate, Volume, Reaction time and Tone were regular. He had an inappropriate emotional expression. His mood was anxious, sad and fearful; anxiety and fear were visible objectively. He had a flight of ideas and circumstantial thoughts, and his content of thought was a delusion of persecution, delusion of reference and thought broadcasting. He had a visual hallucination of a policeman standing in front of his home. He had a good memory for general information and intelligence, with average attention, concentration and abstraction. Insight grade 1.
Diagnostic assessment
Considering all the presenting complaints and his mental status examination, the Consultant Psychiatrist of the Institute diagnosed the case as an Alcohol Withdrawal state with Delirium (F10.4) as per the International Classification of Diseases-10 Diagnostic guidelines.[2] The psychiatrist confirmed the typical symptoms of an Alcohol Withdrawal state with Delirium, which is a consequence of absolute or relative withdrawal of alcohol in severely dependent users with a long history of use.
Therapeutic intervention
Acute totality was framed based on the presentation of the symptoms, and repertorisation was done. The following symptoms were considered for repertorisation: Persecution in delirium, delusion pursued, suicidal disposition with fear of death, restlessness fear from, sleeplessness fear, thirst unquenchable, company desire for alone when aggravation, fear of the dark and suicidal disposition delusion from. Based on the repertorisation, Arsenicum album (Ars. alb) 30 C was prescribed once in 4 h, and it was reduced gradually when the symptoms responded to medicine. The repertorial chart is shown in Figure 1.
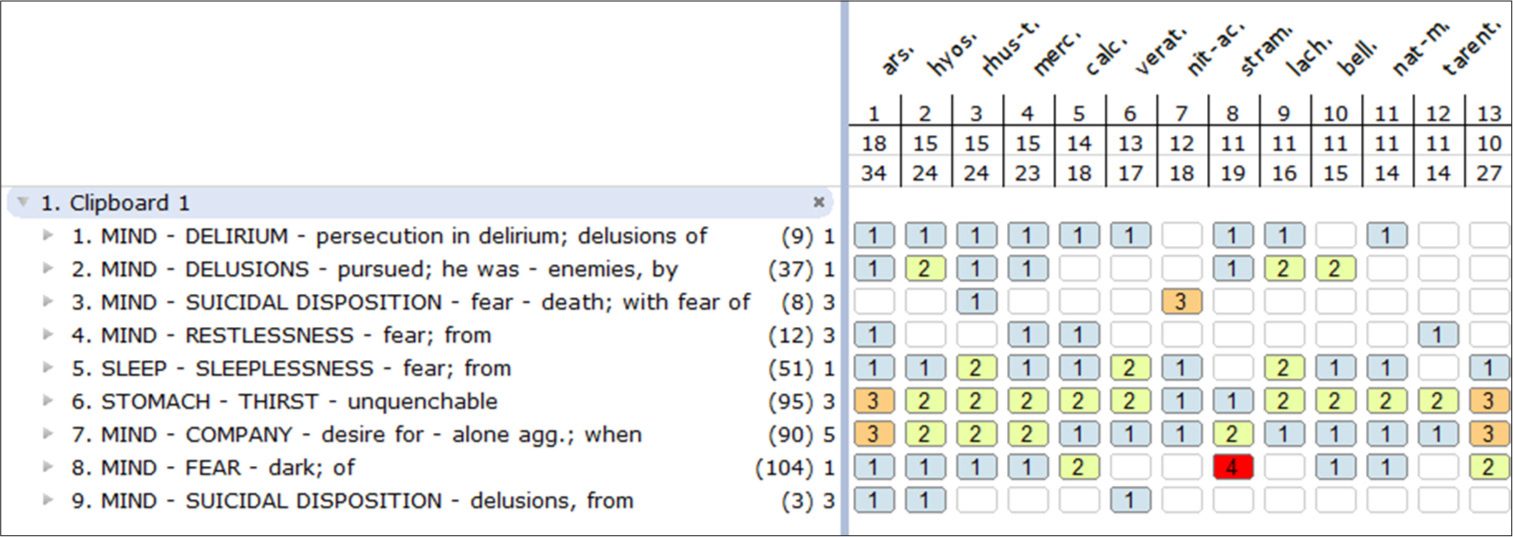
- Repertorial chart. Red colour indicates first grade, orange colour indicates second grade, yellow colour indicates third grade, blue colour indicates four grade.
Follow-up and outcomes
A follow-up of the case and assessment of the scale was carried out for 1 month. The case follow-up is depicted in Table 1. Temporary worsening of pre-existing symptoms was not noticed. Significant improvement in the symptoms was observed, exclusively with homoeopathic medicines.
| Date | Symptoms | Prescription | CIWA score |
|---|---|---|---|
| May 20, 2023 | Sleeplessness, suspicious that someone was coming to kill him. Visual hallucination that a policeman was standing in front of his house. Suspicious that someone listened to whatever they spoke and kept a recorder at home. He was doubtful that he could hear a musical tone and constantly searched for the music-producing device on his pants, under the table, on his body, etc. The patient was admitted to the in-patient department of the institute on May 20, 2023 at 1 p.m. | Ars. alb 30 and blank tablet 3 grain were given TDS (3 times daily) | 16 |
| May 20, 2023 | The patient had a severe headache the same day at 7 p.m. His throbbing pain in both temples was ameliorated by pressing on the temple region. His blood pressure was 170/100 mmHg. | Glon 200/3 dose was prescribed based on throbbing pain, ameliorated by pressure and high blood pressure. Only one dose was taken by the patient, and after an hour, his blood pressure reached 120/80 mmHg, and the headache was relieved. | |
| May 21, 2023 | He had 5 h of sleep, but the remaining symptoms reappeared as such on the following day. | Ars. alb 30 was prescribed once in 4 h, and a blank tablet 3 grains was given TDS | 16 |
| May 22, 2023 | He had a sound sleep. No suicidal and suspicious thoughts. No delusions and hallucinations. Tremor of hands –reduced. Anxiety and fear were under control. His psychomotor activity was under control. | The previous day, he had taken five doses of Ars. alb 30. On May 22, 2023 Ars. alb 30 C was kept as anSOS (only when required). Saclac 3 dose and blank tablet 3 Grain were given TDS | 4 |
| May 23, 2023 | He had a sound sleep. No suicidal and suspicious thoughts. No delusions and hallucinations. Tremor of hands –reduced. Anxiety and fear was under control. His psychomotor activity was under control. | The patient had not taken SOS. Saclac 3 dose and blank tablet 3 grain were given TDS | 2 |
| May 24, 2023 | He had a sound sleep. No suicidal and suspicious thoughts. No delusions and hallucinations. Anxiety and fear were under control. His psychomotor activity was under control. Tremors of hands were completely reduced. | Saclac 3 dose and blank tablet 3 grain were given TDS. | 0 |
| May 25, 2023 | Asymptomatic | Saclac 3 dose and blank tablet 3 Grain were given TDS. | 0 |
| May 26, 2023 | Asymptomatic. Hence, the patient was discharged | Ars. alb 30 C/2 dose was prescribed along with saclac, and blank tablet 3 Grain was given TDS for a week | 0 |
His past follow-up was on July 25, 2023, and during this period, the patient abstained from alcohol, and symptoms did not reappear. He had not taken SOS (only when required) medicine yet. CIWA: Clinical Institute withdrawal assessment, Ars. alb: Arsenicum album, TDS: Three times a day
DISCUSSION
The case report has been presented as per the homoeopathic clinical case reports (HOM-CASE) guidelines.[11] Delirium is an acute emergency with psychiatric symptoms, with 80% of patients admitted to the ICU. If DTs are not recognised early and treated appropriately, it can be fatal.[1] The case falls under the second category of Hahnemannian classification of mental disorders mentioned in the Organon of Medicine.[12] To specify the strength of this case study, his mental symptoms were prominent, and the patient displayed the pre-disposition feature of the Ars. alb. The anxiety, fear and insecurity of the Ars. alb is expressed by its well-known symptoms, such as fear of being alone and dark with a constant need for company. An agonizing fear of death and intense fear accompanied by anxiety. The restlessness and anxiety can be tremendous, compelling the patient to get up and move about.[13] Furthermore, it covers other symptoms, such as delusions and unquenchable thirst.
The patient had a severe headache on May 20, 2023, at 7 p.m. He had pain in both his temples, and his pain was throbbing. The pain was ameliorated by pressing on the temple region. His blood pressure was 170/100 mmHg. Glonoinum (Glon) 200 C was prescribed, and after an hour, his blood pressure reached 120/80 mmHg, and the headache was relieved.
A psychiatrist has diagnosed the case and severity assessment of CIWA-Ar, a universally accepted rating scale. The clinical outcome of the case was assessed with CIWA-Ar, which showed a marked reduction in the intensity of symptoms. The initial score of CIWA-Ar was 16 (moderate category), which gradually reduced to 0 (remission stage), and overall, well-being was offered expeditiously with homoeopathy medicine alone.
The limitation of this case report is the lack of objective evidence, which is challenging to get in psychiatric cases. In this case, the effectiveness of homoeopathic medicine was evidenced only for moderate severity of alcohol withdrawal delirium.
The minutest dose of the medicine is sufficient to effect the necessary change and to excite the vital force for its further action. Furthermore, this simillimum, when repeated at suitable intervals, pronounces the acceleration of cure to the fullest, influencing the vital force towards the effects of treatment.[14]
Early and speedy intervention with appropriate repetition can potentially prevent the deteriorating condition.
CONCLUSION
The favourable outcome in managing alcohol withdrawal delirium was treated exclusively with Homoeopathy medicine using the validated scale CIWA-Ar. Further studies with large sample sizes and rigorous designs are warranted.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that they have used artificial intelligence (AI)-assisted technology to assist in the writing or editing of the manuscript or image creations.
Financial support and sponsorship
Nil.
References
- Alcohol withdrawal delirium-diagnosis, course and treatment. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2015;159:44-52.
- [CrossRef] [PubMed] [Google Scholar]
- The ICD-10, classification of mental and behavioural disorders NewDelhi: A.I.T.B.S. Publishers and Distributors; 2007. p. :78-9.
- [Google Scholar]
- Kaplan and sadock's synopsis of psychiatry: Behavioural sciences clinical psychiatry (7th ed). Williams & Wilkins; 1994. p. :630.
- [Google Scholar]
- Delirium research in India: A systematic review. J Neurosci Rural Pract. 2021;12:236-66.
- [CrossRef] [PubMed] [Google Scholar]
- Delirium tremens In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482134 [Last accessed 2024 Jan 28]
- [Google Scholar]
- Homoeopathic treatment of alcohol withdrawal. Br Homeopathic J. 1993;82:249-51.
- [CrossRef] [Google Scholar]
- Managing acute alcohol withdrawal with homoeopathy: A prospective, observational, multicentre exploratory study. Indian J Res Homoeopathy. 2014;8:224-30.
- [Google Scholar]
- A randomized comparative trial in the management of alcohol dependence: Individualized homoeopathy versus standard allopathic treatment. Indian J Res Homoeopathy. 2016;10:172-81.
- [CrossRef] [Google Scholar]
- Homoeopathic management of acute alcohol withdrawal syndrome: A retrospective cohort study. Am J Homeopathic Med. 2020;113:17.
- [Google Scholar]
- Assessment of alcohol withdrawal: The revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar) Br J Addict. 1989;84:1353-7.
- [CrossRef] [PubMed] [Google Scholar]
- Homoeopathic clinical case reports: Development of a supplement HOM-CASE) to the CARE clinical case reporting guideline. Complement Ther Med. 2016;25:78-85.
- [CrossRef] [PubMed] [Google Scholar]
- Organon of medicine In: Combined (5th and 6th ed). New Delhi: B. Jain Publishers; 2005.
- [Google Scholar]
- New manual of homoeopathic materia medica with repertory (3rd ed). New Delhi: B. Jain Publishers; 2016. p. :72-73.
- [Google Scholar]




