
Translate this page into:
An evidence-based case of bilateral nephrolithiasis treated with individualised homoeopathic medicine: A case report
*Corresponding author: Dr. Kapil Das, M D (Hom.) Regional Research Institute of Homoeopathy, Agartala, Under Central Council for Research in Homoeopathy, Ministry of AYUSH, Agartala, Tripura, India. kapildas11993@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Debnath N, Das K. An evidence-based case of bilateral nephrolithiasis treated with individualised homoeopathic medicine: A case report. J Intgr Stand Homoeopathy. 2024;7:186-91. doi: 10.25259/JISH_70_2023
Abstract
Nephrolithiasis, or renal calculi, is a painful and common urinary disorder affecting millions worldwide. Conventional treatments primarily focus on pain management and calculus removal, but concerns about recurrence have led many patients to seek alternative therapies. Homoeopathy, a holistic medical system, offers an intriguing approach to managing nephrolithiasis. A 35-year-old patient presented with bilateral flank pain radiating up to the groin with an ultrasonography report of non-obstructive bilateral renal calculi. He was treated effectively with the homoeopathic medicine Thuja, which was selected according to case totality. This case shows the efficacy of homoeopathic medicines in addressing and expelling bilateral renal calculi. A large-scale randomised trial is recommended to assess the efficacy of individualised homoeopathic treatment.
Keywords
Nephrolithiasis
Renal calculi
Homoeopathy
Thuja
Case report

INTRODUCTION
Renal calculi are amongst the most prevalent urological issues.[1] Approximately 2% of the population develops renal calculi at some point in their life, with a male-female ratio of 2:1. The highest occurrence is seen in people in their 20s and 30s.[2] Urolithiasis occurs when urine solutes crystallise to form calculi due to factors such as low urine volume, anatomic features causing urinary stasis, dietary factors, infections, acidosis, medications, or genetic factors such as cystinuria. The main cause is inadequate hydration and low urine volume. Other common factors include hypercalciuria, hyperoxaluria, hyperuricosuria and hypocitraturia.[3]
Renal calculi have different types, including calcium, struvite, uric acid, and cystine. Amongst these, calcium is the most common type, with a higher recurrence rate.[4] Calculi can be asymptomatic or cause haematuria; moreover, when they pass, they may cause severe pain radiating from the loin to the groin, accompanied by nausea, vomiting, and light-headedness.
Most renal calculi are small enough to pass spontaneously. However, in case of larger calculi (6–7 mm or larger), extracorporeal shock wave lithotripsy or surgery may be required.[5] Depending on the circumstances, a small calculus (<5 mm) can take 4–6 weeks to pass. However, if it fails to pass spontaneously, the physician can provide appropriate medication, such as an alpha-blocker and calcium channel blocker.[6] Radiography of the kidney-ureter-bladder region detects 90% of radio-opaque renal calculi, while abdominal ultrasonography (USG) can find radiolucent ones. Computed tomography helps locate small missed ureter calculi.[7]
Homoeopathy, which takes a holistic approach to treating the individual as a whole, can play an important role in properly managing renal calculi. According to studies, the disintegration or evacuation of calculi can be positively influenced by homoeopathic treatment. The Central Council for Research in Homoeopathy carried out a prospective, multi-centric observational study[8] to determine the role of homoeopathic therapy in urolithiasis, in which 106 of 220 cases reported the expulsion of calculi. The individualised homoeopathic medicines (IHMs) reported to be effective in this study included Lycopodium clavatum, Sulphur, Pulsatilla nigricans, Nux vomica, and Cantharis.
CASE REPORT
Patient information
A 35-year-old man sought medical attention at the National Institute of Homoeopathy, Kolkata, on 6th December 2021; presented with a complaint of flank pain on both sides that had been persisting for 6 months along with a USG report of non-obstructive bilateral nephrolithiasis. The pain was more pronounced on the left side and extended up to the groin on both sides. The pain was exacerbated before urination and relieved by movement.
History of presenting complaints
The patient was asymptomatic 6 months prior; then, he began experiencing flank pain on the left side, which gradually progressed to both sides. The patient had not sought any treatment for the past few months since the symptoms began. Despite maintaining a healthy diet and consuming plenty of water, his complaints persisted for 6 months, pushing him to seek medical attention.
Personal history
The patient had renal calculi 5 years prior and had been successfully treated with homoeopathic medication for the same.
Family history
No significant family history was found.
Physical generals
The patient has a good appetite but is easily satiated. He craves extra salt and raw onion; he prefers cold food. His thirst is moderate. He experiences a burning sensation during urination; the urine has a strong odour. His stool is often offensive. His perspiration has an offensive odour, more while sleeping. His thermal sensitivity was chilly.
Mental generals
The patient was irritable, easily angered, and desired to work according to his preferences.
Clinical examinations
The blood pressure and pulse were 120/80 mmHg and 77 beats/min, respectively. No significant abnormalities were found on further general examination.
Diagnostic assessment
Ancillary investigation of USG of the whole abdomen indicates multiple small calculi with varying sizes (2.4–3.3 mm) in both kidneys and grade I hepatic steatosis [Figure 1].
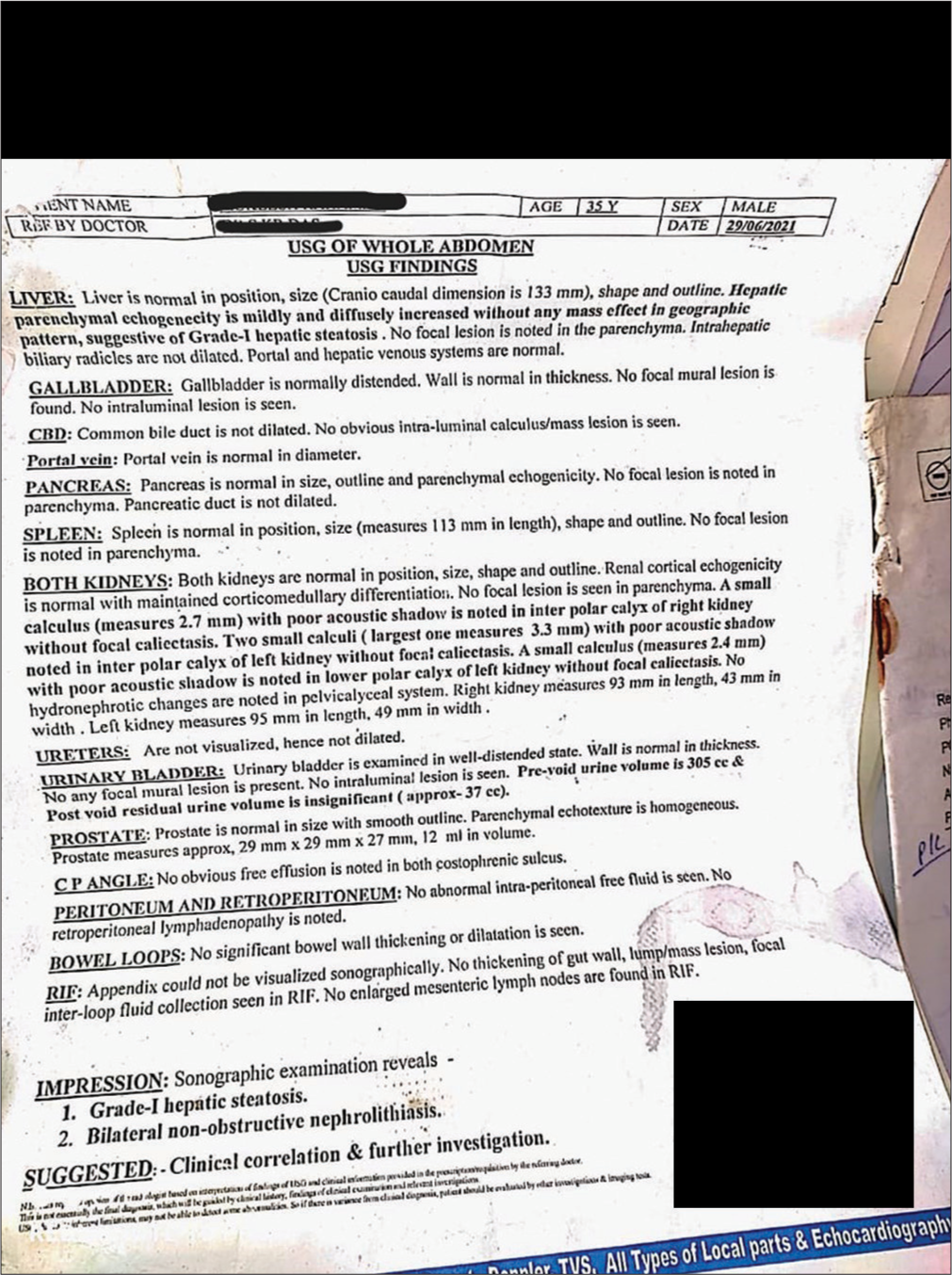
- Ultrasonography report before treatment.
This case was diagnosed as bilateral non-obstructive nephrolithiasis based on the investigation results. The diagnosis was coded GB70.0 according to the International Classification of Diseases, 11th Revision classification; it stands for calculus of the kidney.[9]
Analysis of the case and repertorial result
After conducting a thorough case-taking and analysing all the mental, physical, and particular symptoms, each symptom was evaluated based on its significance [Table 1].
| Characteristic | Irritability. |
| Mental generals | Appetite – easily satiate. |
| Characteristic | Desire – raw onion, salty and cold food. |
| Physical generals | Perspiration – offensive in odour. |
| Particulars | Urination had a strong odour. |
| Thermal relation – chilly. | |
| Burning sensation during urination. | |
| Pain in both lumber regions extending to the groin. | |
| Pain < before burning urination and > by motion. |
In this case, repertorisation was carried out using the Zomeo computer software, using Kent Repertory.[10] After repertorisation, the top-ranked medicines were Thuja (17/8), Phosphorus (16/7), Lycopodium (15/6), and Nitric acid (15/6). The repertorial result is shown in Figure 2.
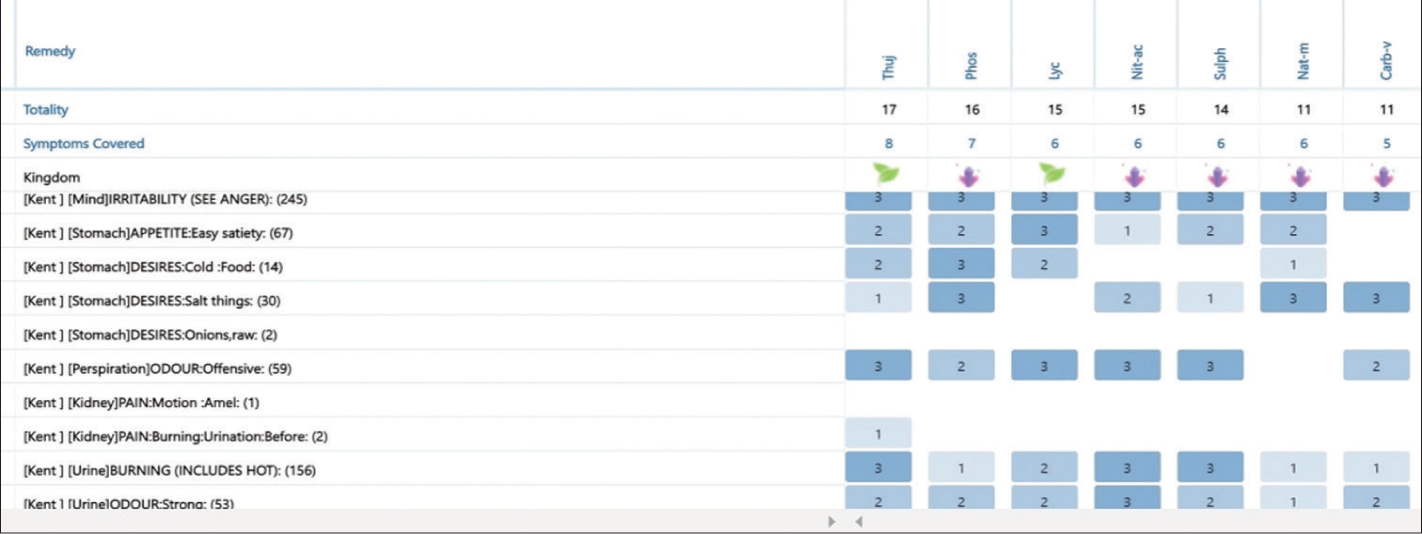
- Repertorial sheet. The numbers in brackets indicate the number of medicines containing that particular symptom. The number 1/2/3 indicates grading of symptoms as per Kent’s repertory.
Therapeutic intervention
Considering the repertorial totality and consultation with Materia Medica, Thuja 0/1 was given on alternative days for 30 days. He was advised to take plenty of water and undergo a urine examination.
Basis of prescription
The patient was irritable, his appetite was good but easily satiated. He has a marked desire for raw onion and prefers cold food. He had a burning sensation during urination with a strong odour. His perspiration has an offensive odour, and his thermal relation is chilly. On repertorial analysis, Thuja stood at the number one position.
The 50 millesimal or LM potency was chosen to avoid undesirable aggravation, which is the main advantage of 50M potencies over CM.[11]
Differentiating points
Phosphorus patients experience hunger even after eating, whereas in this case, the patient was easily satiated. Lycopodium patients desire sweet things and like to take food and drinks hot, whereas in this presented case, the patient desires salty and cold food. In comparison to Thuja, Nitric acid covers fewer symptoms and lacks important symptoms such as desire for raw onion and pain before urination.[12]
Results
Following the use of the homoeopathic medication Thuja 0/1, the patient gradually improved. The drug was continued up to Thuja 0/5, with significant improvement in the manifesting symptoms. Follow-up is summarised in Table 2.
| Date | Observation | Medicine |
|---|---|---|
| First visit December 06, 2021 | Baseline presenting complaints (signs and symptoms) | Thuja 0/1/AD/30 days |
| Second visit January 05, 2022 | Pain in the right side of the flank was better, but on the left side, it was same Burning during urine was occasionally present Generals were good The urine examination report shows that RBC in urine was within normal limits |
Thuja 0/2/AD/30 days |
| Third visit February 08, 2022 | Pain in both sides of flank was better No episodes of burning during urine were observed Generals were good |
Thuja 0/3/AD/30 days |
| Fourth visit March 09, 2022 | Patient was better No episodes of burning during urine were observed Generals were good USG of the whole abdomen and a urine examination were suggested |
Thuja 0/4/AD/30 days |
| Fifth visit April 06, 2022 | No recurrence or worsening of his presenting complaints was observed further. His USG investigation revealed no renal calculi or hepatic steatosis The urine examination report shows no red blood cells in the urine |
Thuja 0/5/AD/30 days |
USG: Ultrasonography, RBC: Red blood cell, AD: Alternate day
The overall duration of treatment with homoeopathic medication was 5 months (from December 06, 2021, to May 06, 2022). The patient was observed for an additional 6 months, and there was no indication of reappearance of symptoms during that period of time.
DISCUSSION
In this case, the patient had bilateral renal Calculi that were successfully treated using homoeopathy. Although these calculi were non-obstructive or small sized, they had been bothering the patient for 6 months, prompting him to seek medical assistance. This case report followed the HOME-CASE guidelines[13] for reporting the outcomes.
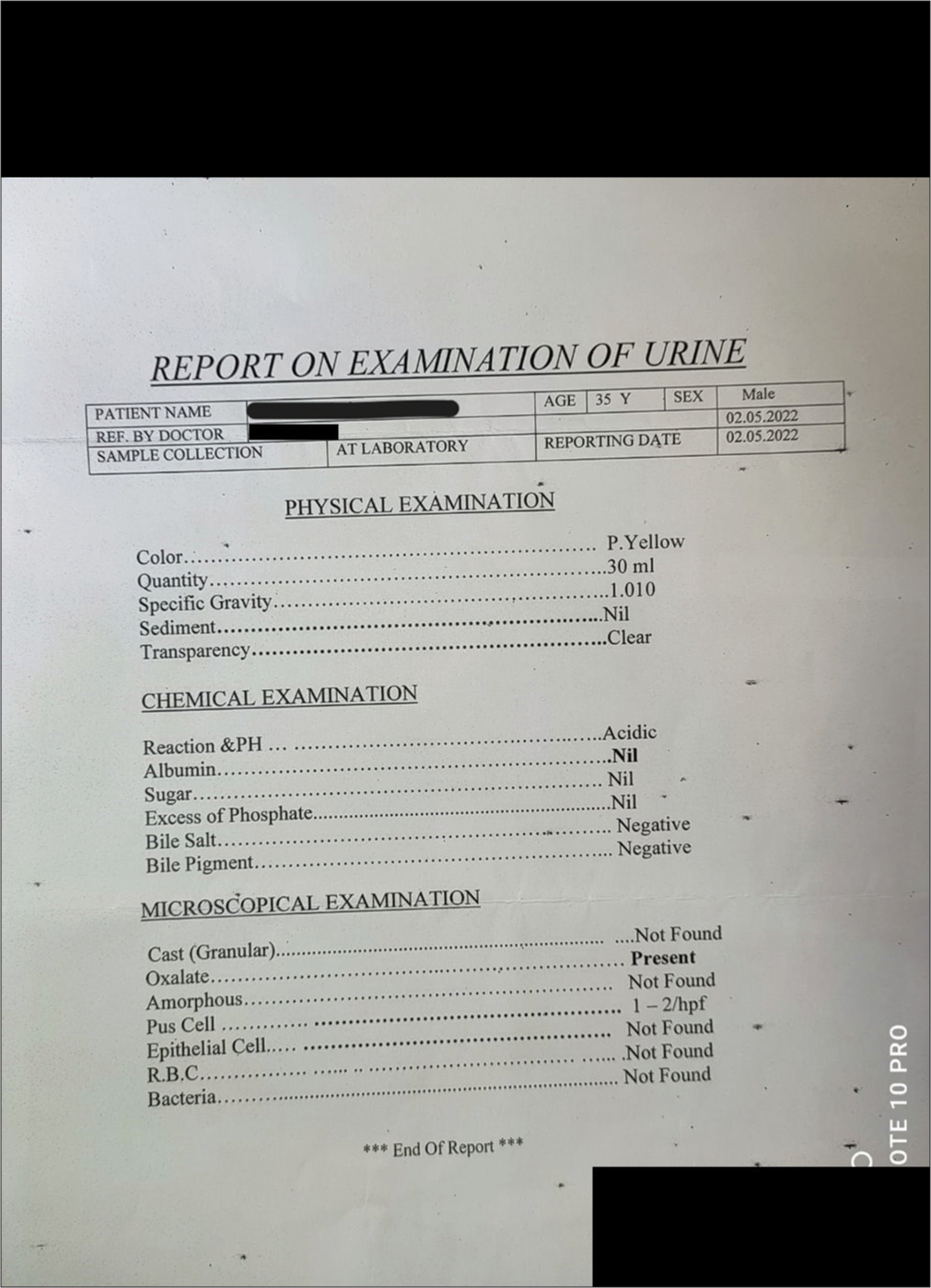
After a detailed case-taking and symptom analysis, Thuja Q1 was selected as the IHM for this case. Urine examination report at second visit (Jan 05, 2022) shows that RBC in urine was within normal limits [Figure 3]. After the initial prescription, the patient began to improve in his presenting issues within 1–2 months, and his complaints were fully resolved after 4 months. Thuja up to 0/5 was maintained, and a USG of the entire abdomen was conducted on May 04, 2022, revealing no renal calculi. Hepatic steatosis or fatty liver also got resolved with the same IHM [Figure 4]. Urine examination was done which shows no red cell in urine [Figure 5]. In one study, homoeopathic treatment was reported to be effective in renal calculi linked with fatty liver.[14]
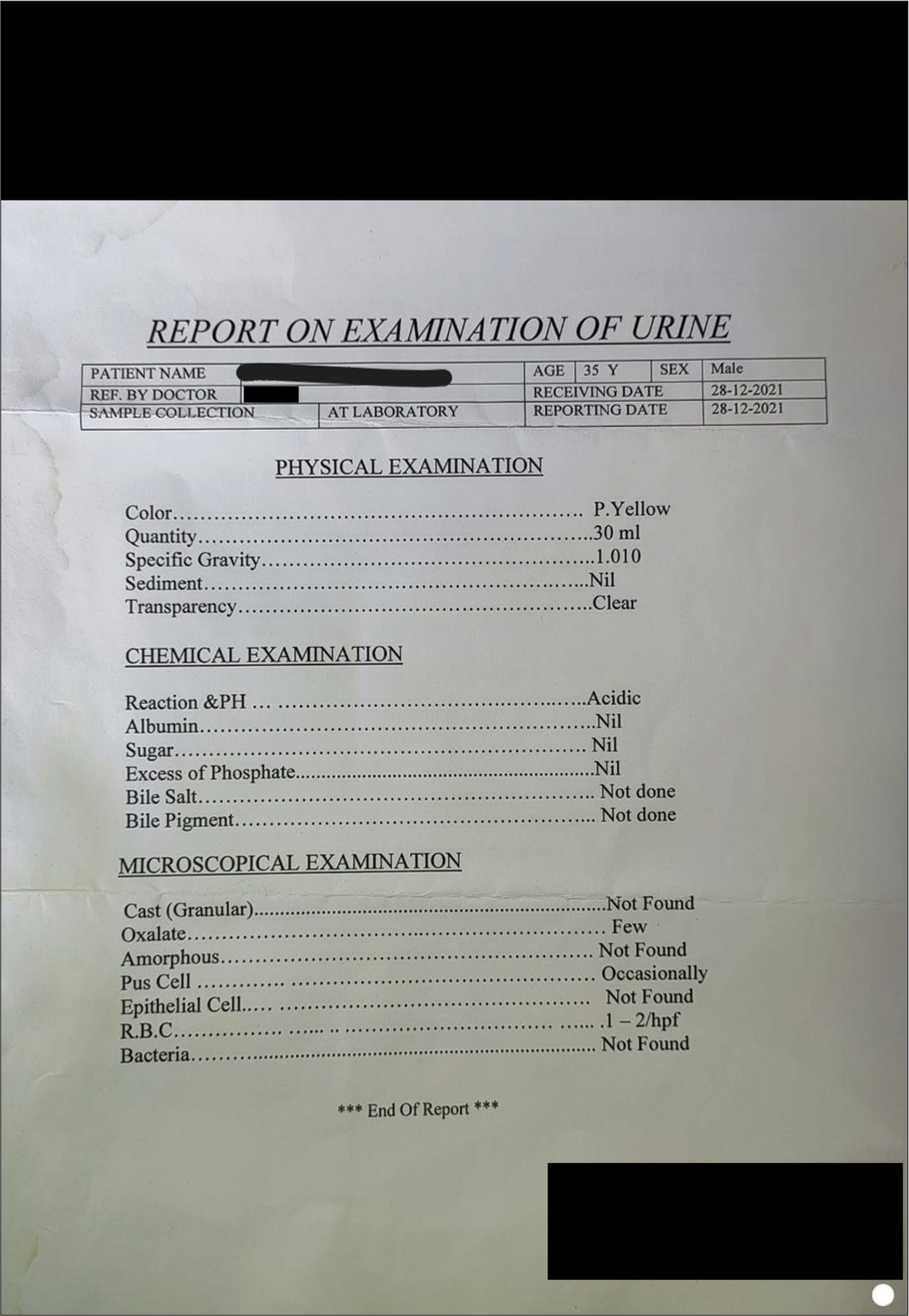
- Urine report before treatment.
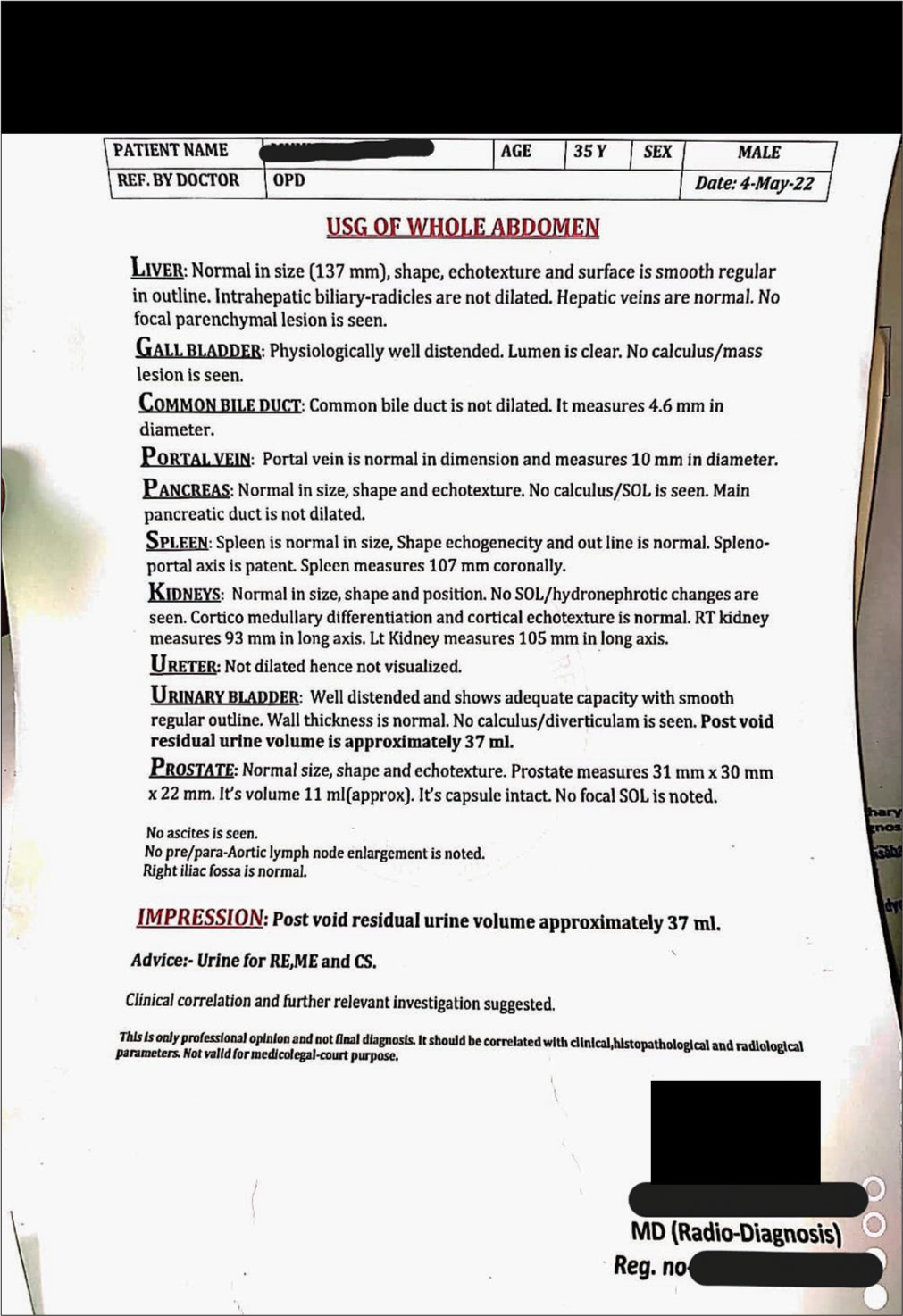
- Ultrasonography report after treatment.
- Urine report after treatment.
There have been several studies that demonstrate positive results in treating cases of renal calculi with homoeopathy.[15-18] Even large urinary calculi (16.9 mm) have also been reported to be eliminated by homoeopathic treatment.[19] The homoeopathic medicine, i.e. Thuja, was also found to be beneficial in the treatment of renal calculi.[20]
The case was assessed using modified Naranjo criteria (MONARCH Inventory),[21] which revealed a positive correlation between homoeopathic treatment and the outcome [Table 3].
| S. No. | Domains | Yes | No | Not sure or N/A |
|---|---|---|---|---|
| 1. | Was there an improvement in the main symptom or condition for which the homoeopathic medicine was prescribed? | +2 | - | - |
| 2. | Did the clinical improvement occur within a plausible time frame relative to the drug intake? | +1 | - | - |
| 3. | Was there a homoeopathic aggravation of symptoms? | - | 0 | - |
| 4. | Did the effect encompass more than the main symptom or condition (i.e. were other symptoms, not related to the main presenting complaint, improved or changed) | +1 | - | - |
| 5. | Did overall well-being improve? (Suggest using a validated scale or mention about changes in physical, emotional, and behavioural elements) | +1 | - | - |
| 6. | Direction of cure: Did some symptoms improve in the opposite order of the development of symptoms of the disease? | - | - | 0 |
| 7. | Direction of cure: Did at least one of the following aspects apply to the order of improvement of symptoms: • From organs of more importance to those of less importance? • From deeper to more superficial aspects of the individual? • From the top downwards? |
- | - | 0 |
| 8. | Did ‘old symptoms’ (defined as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? | - | 0 | - |
| 9. | Are there alternative causes (other than the medicine) that – with a high probability – could have produced the improvement? (Consider the known course of disease, other forms of treatment, and other clinically relevant interventions) | - | +1 | - |
| 10. | Was the health improvement confirmed by any objective evidence? (e.g., investigations and clinical examination) | +2 | - | - |
| 11. | Did repeat dosing, if conducted, create similar clinical improvement? | +1 | - | - |
MONARCH: Modified Naranjo Criteria for Homeopathy, N/A: Not applicable
The approach to managing renal calculi requires a personalised strategy. Evaluating symptoms, medical history, and test results aid in determining the necessity for immediate surgery or medical intervention. For clinically stable individuals with non-obstructive calculi, individuals who frequently develop calculi, and those with underlying systemic conditions, medical management is the recommended course of action.[22] Homoeopathy is a simple system of medicine that focuses on addressing the person as a whole, considering both physical and emotional aspects for effective healing.
CONCLUSION
In this case, multiple renal calculi were present bilaterally and were treated efficiently with IHM. While homoeopathy offers a potentially attractive alternative for managing renal calculi, the current scientific evidence is inconclusive. Further, high-quality research, including well-designed randomised controlled trials, is necessary to determine the true efficacy and safety of homoeopathic remedies in treating renal calculi.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient consent is not required as the patient’s identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Disorders of the kidney and urinary tract- nephrolithiasis In: Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, eds. Harrison’s principles of internal medicine Vol 2. (17th ed). New Delhi: McGraw-Hill Medical Publishing Division; 2008. p. :1815-7.
- [Google Scholar]
- The kidney and lower urinary tract In: Textbook of pathology (5th ed). New Delhi: Jaypee Brothers Medical Publishers Pvt Ltd; 2008. p. :714.
- [Google Scholar]
- Kidney stone disease: An update on current concepts. Adv Urol. 2018;2018:3068365.
- [CrossRef] [PubMed] [Google Scholar]
- Kidney stones. 2023. Available from: https://www.nhsinform.scot/illnesses-and-conditions/kidneys-bladder-and-prostate/kidney-stones#treating-kidney-stones [Last accessed 2023 Aug 08]
- [Google Scholar]
- Small kidney stones. 2023. Available from: https://urologyaustin.com/general-urology/small-kidney-stones [Last accessed 2023 Aug 08]
- [Google Scholar]
- Kidney In: SRB's manual of surgery (4th ed). New Delhi: Jaypee Brothers Medical Publishers Pvt Ltd; 2013. p. :1091.
- [Google Scholar]
- A multicentre observational study to ascertain the role of homoeopathic therapy in urolithiasis. Indian J Res Homoeopathy. 2011;5:30-9.
- [CrossRef] [Google Scholar]
- Eleventh Revision (ICD-11), World Health Organization (WHO) 2019/2021. Available from: https://icd.who.int/browse11 [Last accessed 2023 Nov 01]
- [Google Scholar]
- Repertory of the homoeopathic Materia Medica Uttar Pradesh: B Jain Publishers Pvt Ltd.; 2016.
- [Google Scholar]
- A review on history of LM potency: Tracing its roots in the past. Int J Homoeopath Sci. 2019;3:26-31.
- [CrossRef] [Google Scholar]
- Pocket manual of homoeopathic materia medica with repertory (9th ed). Kolkata: Ghosh Homoeo Pharmacy; 2009. p. 409-510, 643-45
- [Google Scholar]
- Case Reporting in homeopathy-an overview of guidelines and scientific tools. Homeopathy. 2022;111:2-9.
- [CrossRef] [PubMed] [Google Scholar]
- A case report on fatty liver with renal calculi treated with homoeopathy. Int J Homoeopath Sci. 2022;6:41-5.
- [CrossRef] [Google Scholar]
- Scope of homoeopathy in treatment of renal calculi. Int J Homoeopath Sci. 2021;5:246-50.
- [CrossRef] [Google Scholar]
- Individualized homeopathic approach in a case of multiple renal calculi. AYUHOM. 2019;6:80-4.
- [CrossRef] [Google Scholar]
- Management of urolithiasis with individualised homoeopathy-a case report. Indian J Res Homoeopathy. 2021;15:263-9.
- [CrossRef] [Google Scholar]
- Renal calculi: An evidence based case study. Int J Med Allied Heal Sci. 2015;7:5-9.
- [CrossRef] [Google Scholar]
- A big urinary calculus expelled with homoeopathic medicine. Indian J Res Homoeopathy. 2008;2:50-5.
- [CrossRef] [Google Scholar]
- Passage of calculus at lower pole of kidney facilitated by individualised homoeopathy: A case study. Int J AYUSH Case Rep. 2022;6:121-7.
- [Google Scholar]
- Evaluation of the modified Naranjo Criteria for assessing causal attribution of clinical outcome to homeopathic intervention as presented in case reports. Homeopathy. 2020;109:191-7.
- [CrossRef] [PubMed] [Google Scholar]
- Medical management of renal stone. Indian J Endocrinol Metab. 2012;16:236-9.
- [CrossRef] [PubMed] [Google Scholar]




