
Translate this page into:
Cumulative irritant contact dermatitis treated with individualised homoeopathic medicine – An evidence-based case report

*Corresponding author: Dr. Aditi Bhasin, Department of Practice of Medicine, Bakson Homeopathic Medical College and Hospital, Greater Noida, Uttar Pradesh, India. aditi.bhasinbakson@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bhasin A. Cumulative irritant contact dermatitis treated with individualised homoeopathic medicine – An evidence-based case report. J Intgr Stand Homoeopathy. doi: 10.25259/JISH_14_2024
Abstract
Cumulative irritant contact dermatitis (ICD) is caused by multiple episodes of sub-threshold irritant exposure, which, in consequence, disrupts the epidermal barrier, leading to its clinical presentation. A 47-year-old woman presented with maculopapular eruptions and scaling with oozing of white sticky discharge involving the hands and arms. She was diagnosed with cumulative ICD. The patient was treated with individualised homoeopathic medicine using repertorisation, the totality of symptoms and synthesising the results with the theory of elements and the periodic table. Follow-ups were conducted every month, evaluating progress using the Visual Analogue Scale (VAS). At the start of the treatment, the patient reported a VAS score of 07, indicating severe itching. However, after 2 months, this score decreased to 1. To evaluate the response of homoeopathic treatment, the Modified Naranjo Criteria for Homoeopathy-causal attribution inventory were also utilised. This case highlights the effectiveness of individualised homoeopathic medicines in alleviating cumulative ICD. Extensive reporting of similar cases and double-blind placebo-controlled research should be conducted to establish the practical implications of individualised homoeopathic treatment in cumulative ICD.
Keywords
Cumulative irritant contact dermatitis
Eczema
Case taking
Homoeopathic treatment

INTRODUCTION
The term contact dermatitis describes an inflammatory process of the skin that occurs in response to contact with exogenous substances and involves pruritic and erythematous reactions. Irritant contact dermatitis (ICD) is an inflammatory reaction that does not rely on immune sensitisation and can be triggered by various irritants, including those of physical, chemical or mechanical origin.[1] It can be further classified as cumulative, toxic, subtoxic and degenerative. Cumulative ICD occurs due to repeated exposure to subthreshold irritants, which prevents the skin barrier from fully recovering between exposures.[2] The pathophysiology involves exposure to a specific irritant, which leads to disruption of the epidermal barrier, particularly the stratum corneum. This damage increases skin permeability, resulting in trans-epidermal water loss. In addition, the insult caused by the irritant triggers the release of proinflammatory cytokines such as interleukin (IL)-1 alpha, IL-1 beta, IL-6 and tumour necrosis factor-alpha from keratinocytes.[3,4] These cytokines further stimulate the release of proinflammatory mediators, prompting the migration of mononuclear and polymorphonuclear cells to the site of irritant exposure.[2] Both endogenous and exogenous factors contribute to this phenomenon. Endogenous factors, such as skin moisture, anatomical location, age, sweat and sebum production, along with exogenous factors such as detergents and cosmetic products, collectively influence the skin’s natural acidic barrier.
The central belief in homoeopathic medicine is that a remedy capable of inducing similar symptoms in a healthy individual serves as the necessary antidote to alleviate sickness, reinstate harmony in willpower and cognition and effectuate healing in the patient.[5] This treatment paradigm encompasses a comprehensive assessment of the patient’s psychophysical-social axis, considering factors such as their unique physical constitution, moral and intellectual attributes, occupation, lifestyle habits, personal and familial medical history as well as social and domestic relationships. It prioritises the individual suffering from illness over mere nosological disease terms.[6]
CASE REPORT
Chief complaints
A 47-year-old married woman from the Punjabi community, working as a school teacher, presented with the following complaints:
-
Multiple eruptions on both hands with tremendous itching (since 6 months) [Figure 1]
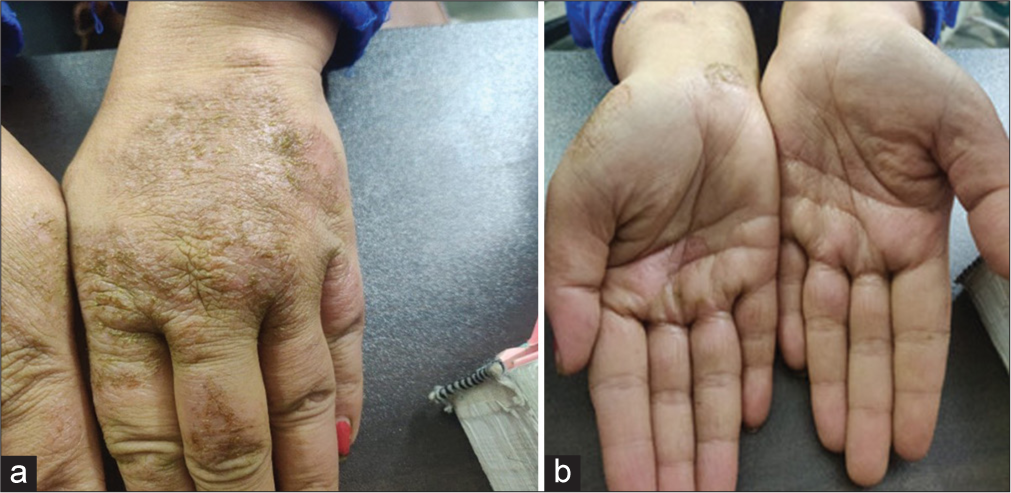 Figure 1:
Figure 1:- Pretreatment status of hand affected with contact dermatitis (a) denotes dorsal aspect of hand, (b) denotes palmar aspect of hand.
Heaviness in the abdomen after eating with loud eructations that persist the entire day (since 6–7 months).
She complains of uncontrollable itching while using water despite changing soaps and detergents many times in the past 6 months. She has also tried avoiding using them (as advised) but even without soap, the slightest contact with water brings back all the complaints.
As exhibited in Table 1 are the presenting complaints of the patient in Location, Sensation, Modalities and Concomitant form as given by Dr Boenninghausen’s.
| Location | Sensation and complaints | Modalities | Concomitant |
|---|---|---|---|
| Skin -dorsal and palmar aspect of both hands and wrist | Itching+++ Burning++White sticky discharge+++ |
Itching+ >scratching |
|
| Duration: Since 6 months O: Sudden Intensity: Moderate to severe |
Associated complaints
As exhibited in Table 2, are the associated complaints of the patient.
| Location | Sensation | Modalities | concomitant |
|---|---|---|---|
| Abdomen | Heaviness + | <after eating+ | |
| Duration: 6–7 months (on and off) Onset: Sudden Intensity: Mild | Burning in retrosternal region+ | <night+ |
Drug history
She had used some topical applications on and off for 6 months; they only temporarily relieved the itching. For the past few days, she has only been applying coconut oil, which alleviates the itching.
Family history
Mother: Deceased (natural death), no history of autoimmune diseases
Father: Deceased (natural death), no history of autoimmune diseases
Brother: Hypertensive (8–9 years)
Daughter: Polycystic ovarian syndrome (since 2 months).
Medical history
No major illnesses such as diabetes, hypertension and thyroid problems.
Menstrual history
Menopause – Surgical (hysterectomy 10 years prior due to fibroids).
Physical generals
As shown in Table 3, the physical generals exhibit few characteristic features which help to individualise the patient.
| Appetite | Decreased (5–6 months), heaviness in abdomen, >walking |
| Desire | Non-veg, especially chicken, spicy food |
| Aversion | None |
| Thirst | 1–2 L/day, thirstless |
| Stool | Hard, difficult to pass on and off for 7–8 years, itching around the anus 2–3 days/unsatisfactory. No episode of bleeding. |
| Urine | D 1–2/N 0–1, no any other associated complaints such as burning and itching |
| Perspiration | Only on exertion, non-offensive, non-staining. |
| Sleep | 6 hours, sound, refreshing |
| Thermally | Chilly |
Appearance – She is fair, flabby, looks older than her age.
Life space
She emphasised the importance of her husband’s support as she confided in him about trivial concerns; minor arguments with people disturb her mentally and she feels best in his calming presence. Despite lacking practical evidence, she also harbours fears of her husband being romantically involved elsewhere, which she believes could devastate her life. She expressed anxiety about the possibility of the disease spreading to other parts of her body, which could potentially hinder her ability to perform daily tasks in the future and this is the thought which brought her to the physician. In addition, she mentioned engaging in regular walks and other activities to maintain her health.
Physical examination
Height: 5’4’
Weight: 80 kg
Gait: Steady
Pallor: Not detected
Icterus: Absent
Cyanosis: Absent
Clubbing: Absent
Lymphadenopathy: Not present
Temperature: Afebrile
Systemic Examination
CNS: Conscious, well oriented
CVS: S1 S2 heard
Respiratory: Air entry bilaterally equal
Abdomen: Soft, non-tender.
Local examination
Skin
Erythematous, multiple maculopapular eruptions with scaling++ and sticky white discharge on the dorsal and palmar aspect of both hands and the wrists.
No other part of the body evolved.
Anorectal examination
The area under examination was smooth free of lesions, swellings, inflammation and tenderness. There was no evidence of mucus on the perianal skin. No additional opening was visualised during the examination.
Differential diagnosis
Atopic d-ermatitis
Cumulative irritant contact dermatitis
Psoriasis.
Diagnostic and clinical assessment
The diagnosis was established from the history of exposure to irritants, while the intensity and duration of the symptoms in the affected area were assessed through clinical examination. Pattern and distribution also played a key role in differentiating this case from other varieties of dermatitis. The Visual Analogue Scale (VAS) was used for assessment. Further, the Modified Naranjo Criteria for Homoeopathy (MONARCH) causal attribution inventory was used to assess the relation of individualised homoeopathic medicine with the outcome.
Diagnostic reasoning
Atopic dermatitis appears early in childhood, occurs mainly on flexor surfaces and is symmetrical in distribution.[7] Moreover, it is characterised by periods of remission and exacerbations; this case history does not depict any childhood presentation and both flexor and extensor surfaces are involved.
Psoriasis is a papulosquamous, immune-mediated disorder of the skin usually associated with systemic involvement.[8] Well-demarcated plaques characterise it with overlying silvery scales.[9]
ICD is the most common type of contact dermatitis. It is the skin’s reaction to the harmful or physical impacts of various environmental substances.[10] History of contact with soaps and detergents indicating repeated exposure for months with bilateral involvement of affected body parts and no history of autoimmune diseases in the family indicates a case of ICD. The final diagnosis was, therefore, cumulative ICD.
Case processing
To compile the comprehensive array of symptoms, an extensive case-taking process was conducted for analysis and evaluation. Mental general, physical general and specific characteristic symptoms were taken into account utilizing Dr Kent’s method of gradation [Table 4].[11] As exhibited in Table 4, is the analysis of the case.
| Symptom classification | Symptoms |
|---|---|
| Mental general | Anxiety about health |
| Mental general | Arguments disturb her Fear something bad will happen |
| Physical general characteristic | Intense itching |
| Physical general characteristic | Itching causing bleeding after scratching |
| Physical general characteristic | Itching<water |
| Physical general characteristic | Whitish sticky discharge, non-offensive |
Totality Repertorial Syndrome (RS)
As exhibited in Figure 2 is the repertorisation sheet of the case analysed using Zomeo Software.
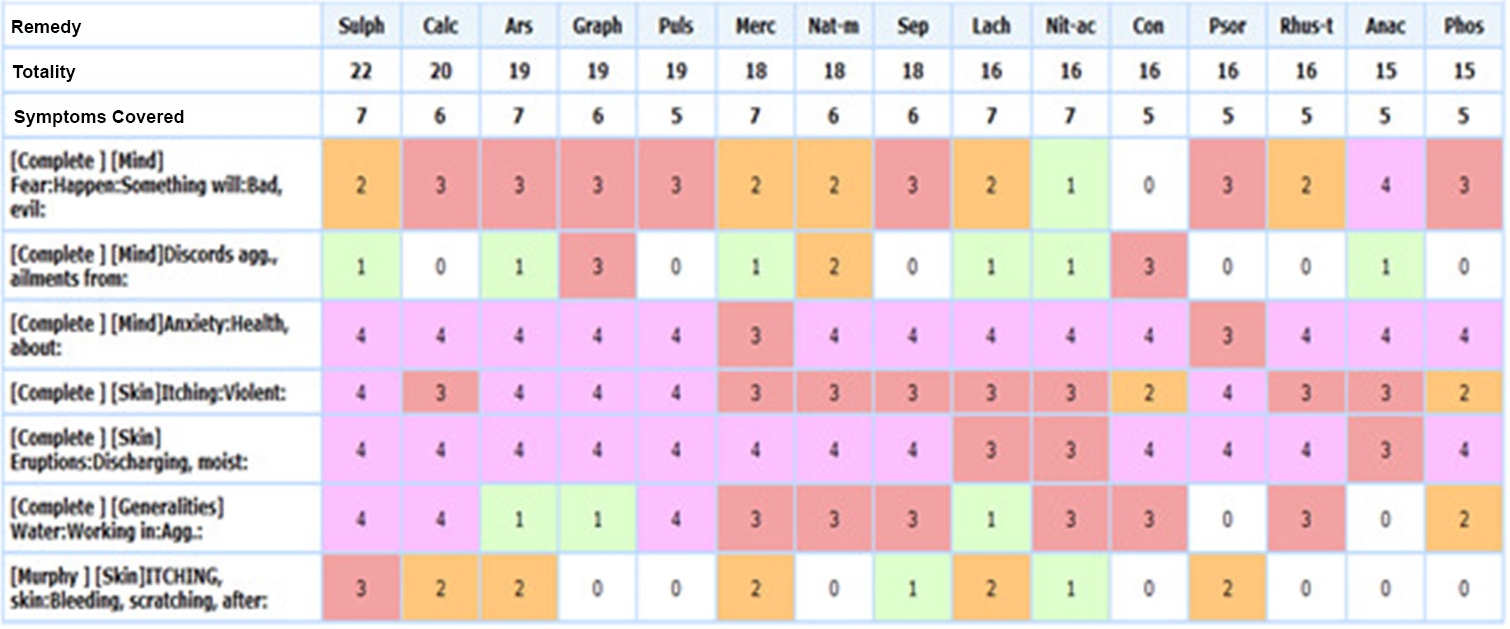
- Repertorisation using Zomeo Software. Significance of color-each color denoted a specific gradation like pink denotes grade 4 symptoms covered by a remedy. Red denotes grade 3, orange denotes 2nd grade and green denotes 1st grade . The color provides the reader a better easy understanding of which remedy covers which symptom in higher grades.
Anxiety about future
Arguments disturb her
Fear something bad will happen
Itching > scratching; Itching < water
Itching is so violent that it causes bleeding
Whitish sticky discharge, non-offensive.
Potential differential field (PDF) for the case
Desire – Chicken++
Thermal- Chilly
These were the two symptoms included in the potential differential field which when added with repertorial totality, should match the conceptual image of the case. Graphites, Calcarea carbonica and Arsenic albums are thermally chilly, whereas Sulphur and Pulsatilla are hot. A desire for chicken is only covered by Graphites among the closely indicated remedies for this case. In referring to Materia Medica, two other remedies cover the desire for chicken (Ferrum iodatum and Phosphorus), but they do not cover the totality of the case.
Remedy differentiation
The remedy was selected using Zomeo Homeopathic Software by Mind Technologies Pvt. Ltd. As the case presented with characteristic mentals and prominent generals, Kent’s approach was used. The repertorisation chart [Figure 2] presents the five closest remedies: Sulphur, Arsenic album, Graphites, Pulsatilla and Calcarea carbonica. Sulphur has the most points (22/7), followed by Pulsatilla (19/5); however, both remedies are thermally hot, which becomes the potential differential field in this case. Arsenic album is characterised by anxiety, restlessness, aggravation by cold, worse 1–2 am, thirst for sips with marked periodicity and deep-seated insecurity, which are absent in this case.[12] Graphites and Calcarea carb are close; Calcarea is chilly, obese and easily exhausted by mental work but has the perseverance to complete the task, whereas Graphites are physically more robust and have an aversion to mental work. Graphites act best in constitutions with a tendency to obesity, which is not of a healthy kind as we find Calcarea showing improper nutrition.[13] However, sweat of the head and cold, damp feet, which are the features of Calcarea are not much prominent under Graphites.[14] Further, Calcarea does not cover a very marked mental general that binds the case of ‘Discords agg, ailments from.’ Desire for chicken is marked in Graphites which is also included in the potential differential field for this case. After final consultation of the repertorisation chart and Materia Medica, Graphites were selected as the final prescription.
Prescription: Graphites 200C single dose.
Materia Medica Differentiation
Graphites have the carbon element which belongs to the second series of the periodic table, whose theme is of events after conception causing separation from the mother. In this series, Boron is confused about whether he is connected to the mother; carbon fears not being able to survive on his own.[15] In this case, this is reflected in the patient’s thought process, as she feels she cannot survive without her husband’s support. Furthermore, the themes of columns thirteen and fourteen reflect their structure to be under attack and loss is unavoidable.[15] They need to make a superhuman effort to maintain it; if it progresses, they understand they have failed and nothing can be done. These shades reflected by the patients fall in these themes and thus, Graphites were selected amongst all the remedies.
The individual requiring Graphites is often affected by grief, especially if it is a woman. She experiences heightened anxiety and apprehension, often fearing imaginary accidents looming on the horizon.[16] This constant state of unease leads to restlessness and an inability to stay in one place. She cannot find solace and is compelled to move about constantly. This anxious disposition, coupled with low spirits, is a hallmark symptom of Graphites.[16]
The Graphites patient struggles with indecision, feeling apprehensive and despondent. This remedy addresses constipation, particularly when accompanied by large, knotty stools coated in mucus threads. In addition, Graphites relieve discomfort in the anus, characterised by smarting, soreness and itching.[17] Skin issues such as oozing, sticky exudation and rough, hard and persistently dry patches unaffected by eczema also respond well to Graphites.
Justification of the selected potency
The potency was moderate to high; this was determined based on the relatively young age of the patient, with the availability of characteristic generals (mental and physical) and particulars. The pathology of the presented case is structurally reversible and the disease progress was insidious. Thus, Graphites were administered in the 200C potency.
Assessment according to MONARCH inventory [Table 5]. As exhibited in Table 5 is the MONARCH causal attribution inventory.
| Domains | Yes | No | Not sure or N/A |
|---|---|---|---|
| 1. Was there an improvement in the main symptom or condition for which the homoeopathic medicine was prescribed? | ✓ | ||
| 2. Did the clinical improvement occur within a plausible time frame relative to the drug intake? | ✓ | ||
| 3. Was there an initial aggravation of symptoms? | |||
| 4. Did the effect encompass more than the main symptom or condition (i.e., were other symptoms ultimately improved or changed)? | ✓ | ✓ | |
| 5. Did overall well-being improve? (suggest using validated scale) | ✓ | ||
| 6A Direction of cure: did some symptoms improve in the opposite order of the development of symptoms of the disease? | ✓ | ||
| 6B Direction of cure: did at least two of the following aspects apply to the order of improvement of symptoms: –from organs of more importance to those of less importance? –from deeper to more superficial aspects of the individual? –from the top downwards? |
✓ | ||
| 7. Did ‘old symptoms’ (defined as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? | ✓ | ||
| 8. Are there alternate causes (other than the medicine) that –with a high probability – could have caused the improvement? (Consider known course of disease, other forms of treatment and other clinically relevant interventions) | ✓ | ||
| 9. Was the health improvement confirmed by any objective evidence? (e.g., laboratory test, clinical observation, etc.) | |||
| 10. Did repeat dosing, if conducted, create similar clinical improvement? | ✓ | ✓ | |
| Total Score – 08 |
MONARCH: Modified Naranjo Criteria for Homoeopathy, N/A: Not available, ✓Denotes the chosen option of MONARCH criteria
DISCUSSION
Dermatology is a branch of medicine where homoeopathic medicines have already solidified their presence. While numerous dermatological conditions are reported in homoeopathic literature, contact dermatitis is quite common. However, very few cases of cumulative ICD are available in the database of Google Scholar and PubMed from 2016 to 2023. Dermatitis is immensely challenging for a homoeopathic physician to manage; patients are quite impatient when dealing with skin complaints, as it not only affects the appearance but also may cause physical discomfort.
This case treated with individualised homoeopathic medicine showed improvement [Figure 3] assessed using the VAS and MONARCH scores. External applications were not used in this case, as Dr Hahnemann outlined in 185 the treatment for local diseases., The aphorism emphasises that the remedy administered must not only match the nature of the specific local afflictions but also correspond to the entirety of symptoms displayed by the patient. The medicine was not changed in this case. The VAS score was initially 7 and reduced 1, which was when treatment was stopped [Table 6]. As exhibited in Table 6 is the timeline of the patients followup with response of patient and the prescriptions.
| S. No | Date | Response of patient | Prescription |
|---|---|---|---|
| 1. | March 12, 2023 | There was no change. Itching was very intense. The patient was restless about getting cured. | Graphites 200, 1 dose stat Placebo 5 pills BD×1 month. |
| 2. | April 18, 2023 | Itching was much better. No bleeding. Gastric complaints were also better. |
Placebo 5 pills TDS×1 month |
| 3. | May 20, 2023 | Itching reduced further, no bleeding. No gastric complaints reported. |
Placebo 5 pills TDS×1 month |
BD: Twice a day, TDS: Thrice a day
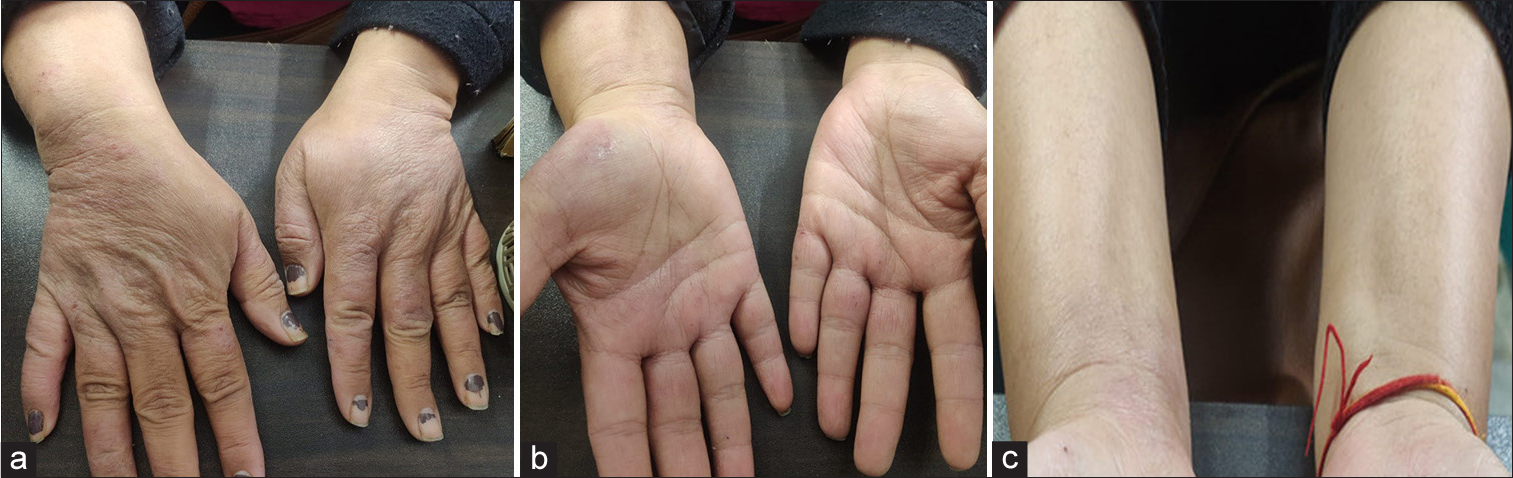
- post treatment status of hand affected with contact dermatitis, (a) denotes dorsal aspect of hand, (b) denotes palmar aspect of hand, (c) denotes palmar aspect of wrist.
Moreover, the evolution of homoeopathic medicine has led to various schools of thought regarding the prescription. In this case, however, the principles laid by Dr. Hahnemann were applied to bring promising results. The principles of totality, repertorisation and Materia Medica differentiation presented by various stalwarts were used to select the prescribed remedy. Synthesising the periodic table was used to confirm Graphites as the similimum.
CONCLUSION
The presented case highlights the successful treatment of cumulative ICD along with improvement noted in the VAS score with individualised homoeopathic medicines. As it elucidates the role of homoeopathy in said diagnosis, this case report may pave the way for further elaborative and well-designed research.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Contact dermatitis: Allergic and irritant. Clin Dermatol. 2014;32:116-24.
- [CrossRef] [PubMed] [Google Scholar]
- Occupational allergic contact dermatitis caused by sterile non-latex protective gloves: Clinical investigation and chemical analyses. Contact Dermatitis. 2013;68:103-10.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiological data on consumer allergy to p-phenylenediamine. Contact Dermatitis. 2008;59:327-43.
- [CrossRef] [PubMed] [Google Scholar]
- Methylisothiazolinone contact allergy: A review. Br J Dermatol. 2011;165:1178-82.
- [CrossRef] [PubMed] [Google Scholar]
- Guideline contact dermatitis: S1-Guidelines of the German contact allergy group (DKG) of the German dermatology society (DDG), the information network of dermatological clinics (IVDK), the German society for allergology and clinical immunology (DGAKI), the working group for occupational and environmental dermatology (ABD) of the DDG, the medical association of German allergologists (AeDA), the professional association of German dermatologists (BVDD) and the DDG. Allergo J Int. 2014;23:126-38.
- [CrossRef] [PubMed] [Google Scholar]
- Translated In: Boericke W, ed. Organon of medicine (6th ed). New Delhi: B. Jain Publishers; 1921.
- [Google Scholar]
- Thoughts on irritant contact dermatitis. Contact Dermatitis. 1981;7:238-47.
- [CrossRef] [Google Scholar]
- Contact dermatitis: Classifications and management. Clin Rev Allergy Immunol. 2021;61:245-81.
- [CrossRef] [PubMed] [Google Scholar]
- A dictionary of practical materia medica. Vol 1. New Delhi: B. Jain Publishers (P) Ltd.; 2013. p. :3534.
- [Google Scholar]
- Allen’s keynotes and characteristics with comparison with bowel nosodes (10th ed). New Delhi: B. Jain Publisher (P) Ltd.; 2005.
- [Google Scholar]




