
Translate this page into:
Hyperuricaemia treated with individualised homoeopathy: A case series
*Corresponding author: Pooja Gautam, Research Officer, Homoeopathic OPD Centre of Central Council for Research in Homoeopathy, Under Ministry of AYUSH at Lady Hardinge Medical College, New Delhi, India. dr.poojagautam@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gautam P, Goel M, Gogoi J. Hyperuricaemia treated with individualised homoeopathy: A case series. J Intgr Stand Homoeopathy. 2024;7:34-45. doi: 10.25259/JISH_25_2023
Abstract
Hyperuricaemia is defined as an elevated level of uric acid in the blood ≥6 mg/dL in women and ≥7 mg/dL in men. If uric acid levels remain high for a longer period, it can lead to gout and nephrolithiasis. Hyperuricaemia is also closely related to other diseases, such as metabolic syndrome, diabetes mellitus, cardiovascular disease and chronic renal disease. Treatment is required to prevent further diseases and complications. This is a case series of three patients with hyperuricaemia who were treated with individualised homoeopathic medicines. The improvement was significant, with a reduction in serum uric acid levels and changes in the measure yourself medical outcome profile two scores. The possible causal attribution of changes was explicitly depicted in each case using the modified Naranjo criteria. Homoeopathic medicines such as Ledum palustre, Nux vomica and Lycopodium were found to be useful.
Keywords
Gout
Homoeopathy
Hyperuricaemia
MYMOP 2
Serum uric acid

INTRODUCTION
Hyperuricaemia is a metabolic disorder defined as serum uric acid concentration ≥7.0 mg/dL (range: 2–7 mg/dL) in men and ≥6.0 mg/dL in women (range: 2–6 mg/dL).[1] The prevalence of hyperuricaemia has increased steadily worldwide in the past 40 years, with higher prevalence in Asian countries, including Taiwan (10–52%), India (25.8%), Japan (20–26%) and China (6–25%) in comparison to the USA (21–22%), Brazil (13%) and Italy (9–12%).[2] Hyperuricaemia does not indicate a pathological state in itself, but if uric acid levels remain high for longer periods, it can lead to several other diseases, such as hypertension, cardiovascular disease, chronic kidney disease and diabetes.[3,4]
The primary method of controlling hyperuricaemia is through monitoring and reducing uric acid levels. European guidelines suggest serum uric acid levels ≤6 mg/dL in people having chronic hyperuricaemia with urate deposition.[5] Conventional treatment of hyperuricaemia includes changes in lifestyle, nutrition and adjunctive therapies, as well as urate-lowering drugs such as xanthine oxidase inhibitors, uricosuric agents and uricase agents. The available urate-lowering drugs have very different efficacies; moreover, tolerability/safety profile and treatment persistence are key factors for a positive clinical outcome.[6]
The homoeopathic system of medicine is a gentle way of healing with the least side effects and without any drug dependency. Homoeopathic literature has many medicines listed for this condition under rubrics such as ‘Uric acid diathesis’, ‘lithemia’, ‘arthritic nodosities’, ‘pain joints, gouty’, ‘acute gout’, ‘nodosities’, ‘tophi’ and ‘Podagra’. However, published evidence in scientific databases such as PubMed, Google Scholar and AYUSH Research Portal reveal a paucity of documentation except for a few case reports[7-9] and very few clinical trials.[10-17]
Here, we report a series of three cases of hyperuricaemia treated in the outpatient department of the Regional Research Institute of Homoeopathy, Agartala, with individualised homoeopathic medicines. To assess the improvement, serum uric acid levels and a patient-centred outcome scale – the measure yourself medical outcome profile 2 (MYMOP 2) were used.[18] The modified Naranjo criteria were used to assess causal attribution between the cause and effect to determine that the improvements resulted from individualised homoeopathic medicines and not any other causes.
CASE SERIES
Case 1
Patient information
The patient was a 46-year-old man with a wheatish complexion and endomorphic build. He was a government employee who reported pain in the smaller joints of the hands and feet for 3–4 years. The pain was dull, aching in character, tolerable to the patient and did not hamper his daily work. The pain was sometimes aggravated after eating meat. Another complaint was frequent gastric disturbances in the form of flatulence and constipation with ineffectual urging for stools on and off for 2–3 years. The flatulence generally worsened in the morning. He occasionally took purgatives and antacids for his gastric complaints. The patient was a known case of diabetes mellitus, diagnosed three months prior and was taking regular conventional treatment for the same along with dietary management. His family history revealed that his father also had diabetes. He had an intolerance for tea, which aggravated his flatulence. The patient used to take alcohol occasionally, although he was not addicted to it. He had a desire for fatty, spicy food even though he could not tolerate it well. His sleep was disturbed; he could not sleep again if he woke once at night. His thermal reaction was chilly. He perspires on exertion, especially his forehead and upper lip. Mentally, the patient was short-tempered and highly irritable. He was very ambitious and studious since childhood.
Clinical findings
Physical examination revealed pre-hypertension (blood pressure [BP]: 136/86 mm Hg), normal pulse rate (78 bpm) and temperature of 97.7℉. His body mass index (BMI) was 27 kg/m2 (weight 77 kg and height 168 cm). His tongue was coated white at the centre. There were no signs of inflammation in the affected joints. After analysing the symptoms, characteristic mental and physical generals considered for totality were pain in joints worse after eating meat, habitual constipation with ineffectual urging for stools, flatulence < morning, tea, fatty, spicy food, desire fatty, spicy food, disturbed sleep, chilly patient, irritable, short-tempered and ambitious.
Diagnostic assessment
Blood biochemical screening was done. Laboratory reports [Figure 1] revealed high serum uric acid levels (7.8 mg/dL) with controlled blood sugar levels (fasting levels 70 mg/dL), marginally elevated serum creatinine level (1.7 mg/dL) and raised serum triglyceride (432 mg/dL) and very low-density lipoprotein (86 mg/dL) levels.
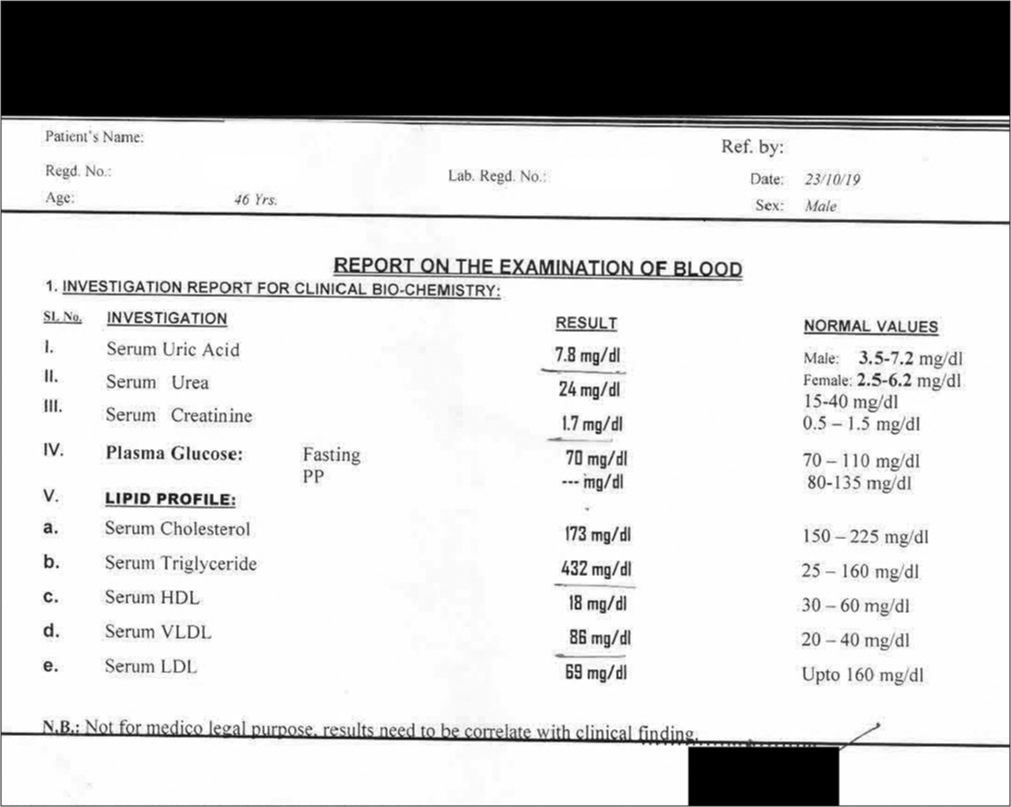
- Blood examination report of Case 1 on 23/10/2019. *HDL: High-density lipoprotein, LDL: Low-density lipoprotein, VLDL: Very low-density lipoprotein
Therapeutic intervention
Repertorial analysis was done using Synthesis 9.0 (SE90) repertory in RADAR 10 software (Schroyens F. RADAR 10, Archibel Homoeopathic Software). The repertorisation chart is presented in Figure 2. The medicines with maximum scores were Nux vomica, Lycopodium, Natrum muriaticum, Argentum nitricum and Arsenic album. As Nux vomica covered the highest marks and the patient was chilly and irritable with a history of taking purgatives/antacids and stimulants, Nux vomica was selected to begin the treatment.
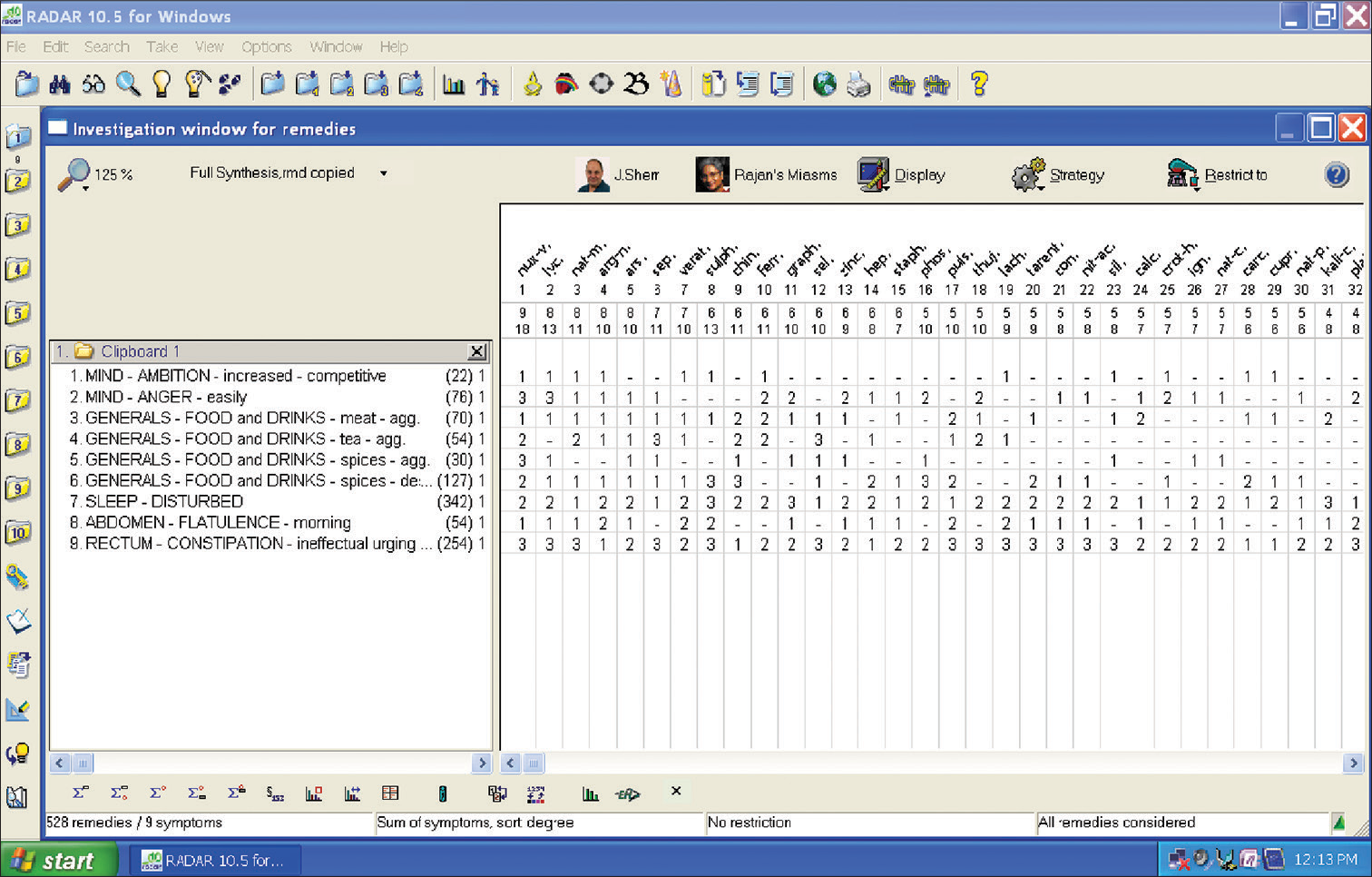
- Repertorisation chart of case no. 1.
The possible causal attribution of the treatment outcome was assessed using the modified Naranjo Criteria as proposed by the HPUS clinical data working group [Table 1]. The total obtained score of 09 reflects that there is a probability that improvement in the patient is attributed to the homoeopathic medicine administered. The MYMOP 2 score was 4.25 at the baseline and 1.25 after the treatment. Follow-up of the patient along with reports [Figures 3-5] were assessed as per the requirement of the case [Table 2].
| Item | Case 1 | Case 2 | Case 3 |
|---|---|---|---|
| Was there an improvement in the main symptom or condition | +2 (Y) | +2 (Y) | +2 (Y) |
| for which the homoeopathic medicine was prescribed? | |||
| Did the clinical improvement occur within a plausible time frame relative to the drug intake? | +1 (Y) | +1 (Y) | +1 (Y) |
| Was there an initial aggravation of the symptom? | 0 (N) | 0 (N) | 0 (N) |
| Did the effect encompass more than the main symptom or condition, i.e., were other symptoms ultimately improved or changed? |
+1 (Y) | +1 (Y) | +1 (Y) |
| Did overall well-being improve? | +1 (Y) | +1 (Y) | +1 (Y) |
| The direction of cure: did some symptoms improve in the opposite order of the development of symptoms of the disease? |
+1 (Y) | +1 (Y) | +1 (Y) |
| The direction of cure: did at least two of the following aspects apply to the order of improvement of symptoms | 0 (N) | +1 (Y) | 0 (N) |
| • From organs of more importance to those of less importance | |||
| • From deeper to more superficial aspects of the individual | |||
| • From the top downwards. | |||
| Did old symptoms (defined as non-seasonal and non-cyclical that were previously thought to have resolved) reappear temporarily during improvement? | 0 (N) | 0 (N) | 0 (N) |
| Are there alternate causes (other than the medicine) that with a high probability- could have caused the improvement? (consider the known course of the disease, other forms of treatment and other clinically relevant interventions) |
0 (NS) | 0 (NS) | 0 (NS) |
| Was the health improvement confirmed by any objective evidence? (e.g. laboratory test and clinical observation) | +2 (Y) | +2 (Y) | +2 (Y) |
| Did repeat dosing, if conducted, create similar clinical improvement? | +1 (Y) | +1 (Y) | +1 (Y) |
| Total | 09 | 10 | 09 |
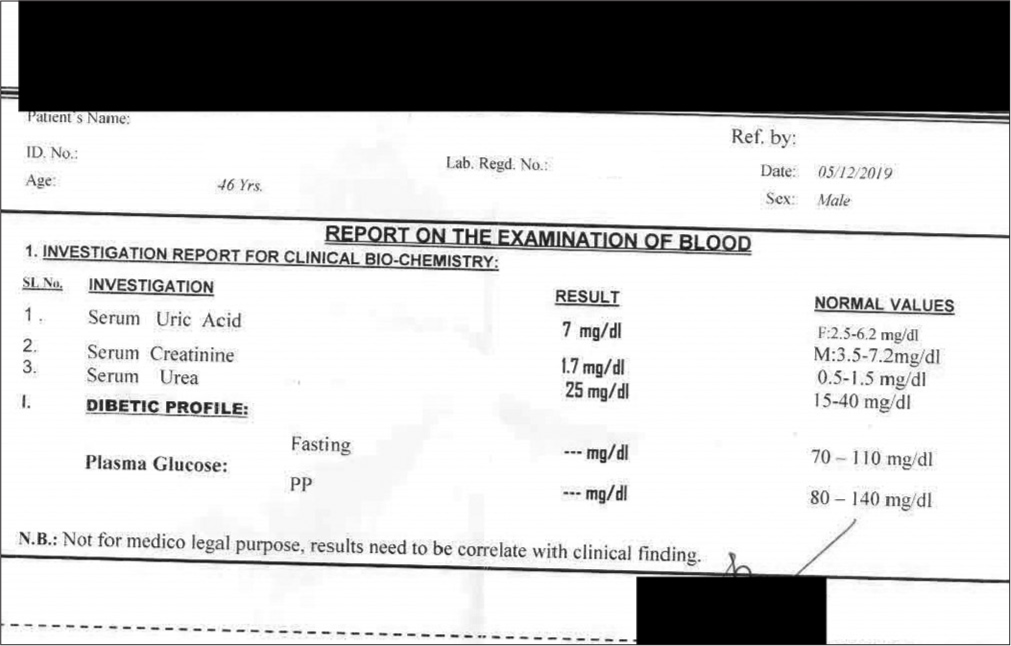
- Blood Examination report of Case 1 on 05.12.2019.
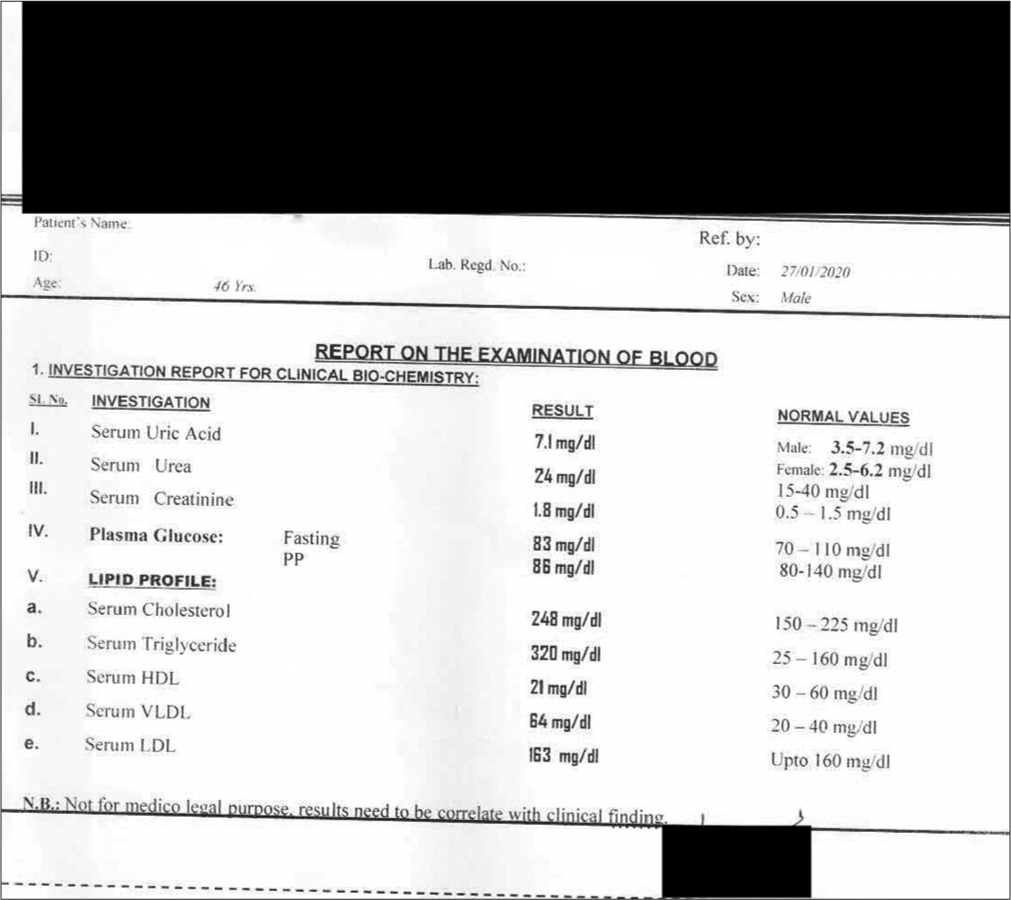
- Blood examination report of Case 1 on 27.01.2020. HDL: High-density lipoprotein, LDL: Low-density lipoprotein, VLDL: Very low-density lipoprotein.
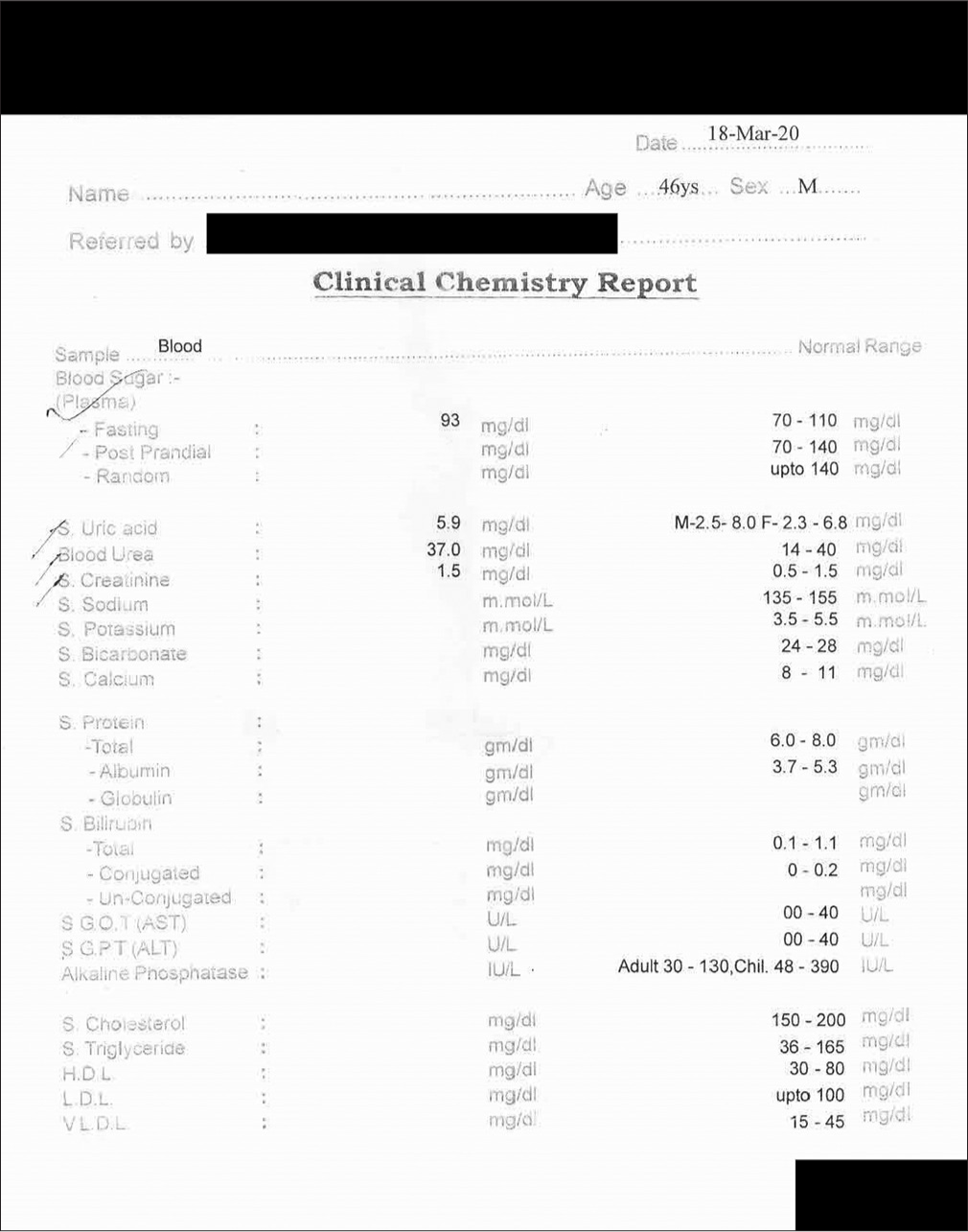
- Blood examination report of case 1 on 18.03.2020. HDL: High-density lipoprotein, LDL: Low-density lipoprotein, VLDL: Very low-density lipoprotein, SGOT: Serum glutamicoxaloacetic transaminase, SGPT: Serum glutamic pyruvic transaminase.
| Date | Symptoms | Laboratory values | Prescription | MYMOP 2 score |
|---|---|---|---|---|
| 17/10/2019 (1st visit, baseline) |
Pain in smaller joints, flatulence, constipation with ineffectual urging. BP: 136/86 mm Hg | Advised: Complete blood count, lipid profile, blood sugar - fasting and postprandial, kidney function test, serum uric acid. |
Nux vomica 30/TDS/3 days; Placebo 30/TDS/14 days |
4.25 |
| 28/10/2019 | Pain in smaller joints was better, flatulence better and ineffectual urging for stools decreased. Considering the good initial response, a placebo was prescribed. BP: 134/86 mm Hg |
Serum uric acid on 23/10/19 [Figure 1]: 7.8 mg/dL, serum triglycerides: 432 mg/dL with raised VLDL: 86 mg/dL. |
Placebo 30/TDS/7 days | 3.25 |
| 05/11/2019 | Flatulence was relieved completely, and ineffectual urging for stools was much better. No further improvement in pain in smaller joints. The patient improved in general, so a placebo was administered. |
Placebo 30/TDS/14 days | 2.75 | |
| 30/11/2019 | Pain in smaller joints same. Flatulence since yesterday. History of eating spicy fatty food at a party. |
Serum uric acid was advised. |
Nux vomica 30/TDS/4 days. Placebo 30/TDS/14 days |
3.5 |
| 23/12/2019 | Pain in smaller joints same. Flatulence relieved. Ineffectual urging for stools was better. |
Serum uric acid on 05/12/19 [Figure 3]: 7.0 mg/dL |
Nux vomica 200/1 dose; Placebo 30/TDS/14 days |
2.75 |
| After the acute symptoms subsided, one dose in higher potency for deeper action was repeated. |
||||
| 16/01/2020 | No further relief and one more dose was repeated. |
Serum uric acid was advised. |
Nux vomica 200/1 dose; Placebo 30/TDS/14 days |
2.75 |
| 01/02/2020. | The condition was at a standstill Hence, higher potency of the same medicine prescribed. BP: 130/84 mm Hg. |
Serum uric acid on 27/01/20 [Figure 4]: 7.1 mg/dL, serum triglycerides: 320 mg/dL, with raised VLDL: 64 mg/dL (improved from previous reports) |
Nux vomica 1M/1 dose; Placebo 30/TDS/14 days |
2.75 |
| 26/02/2020 | Marked improvement in flatulence and constipation. Pain in joints same. Serum uric acid was advised. |
Serum uric acid was advised. | Placebo 30/TDS/14 days | 2.25 |
| 04/03/2020 | Pain in joints same. No further improvement. Hence, one more dose was repeated. |
Serum uric acid was advised again. |
Nux vomica 1M/1 dose; Placebo 30/TDS/14 days |
2.00 |
| 18/05/2020. | Pain in joints disappeared completel0079 The patient was feeling much better overall. BP: 126/80 mm Hg. |
Serum uric acid on 18/03/20 [Figure 5]: 5.9 mg/dL. |
Nux vomica 1M/1 dose; Placebo 30/TDS/14 days |
1.25 |
MYMOP 2: Measure yourself medical outcome profile 2, BP: Blood pressure, VLDL: Very low-density lipoprotein
Case 2
Patient information
A 30-year-old woman with a fair complexion and ectomorphic build reported with pain in the right ankle joint for one month. She also complained of on-and-off dull, aching low back pain for five years radiating toward her right knee and was worse lying on her right side after exertion and relieved by warmth. She was well one month prior when she started developing pain in the right ankle joint with the sensation of heaviness. There was no history of any trauma. She consulted a physician who advised checking the serum uric acid levels; hyperuricaemia was detected. Her spine radiograph (lumbosacral region) was also normal. The patient wanted to take homoeopathic medicines; she was maintaining all the dietary restrictions as advised. She also reported occasional burning while urination, mostly before menses. Family history was insignificant. Her menses were usually delayed with normal flow. Her appetite and thirst were moderate, but she always preferred only hot food. Her thermal reaction was hot, and she used to wear minimal clothing in winter. She complained of flatulence frequently, generally in the evening. Her sleep was refreshing, but she had frequent dreams of accidents, which terrified her. The patient was soft-spoken and shy. Physically, she had a narrow chest with a broader pelvis; the lower part of her body was heavier than the upper part.
Clinical findings
Her physical examination revealed no abnormality with normal BP and pulse rate (BP: 118/78 mm Hg; pulse: 68 beats/min). Her BMI was 20 kg/m2 (weight 50 kg and height 157 cm). Her tongue was clean. No signs of inflammation were seen in the affected joint. She was already a known case of hyperuricaemia. After analysis of symptoms, characteristics generals and particular symptoms considered for the totality include shyness, dreams of accidents, desire for hot food, delayed menses, burning urination before menses, and hot thermal reaction and flatulence in the evening.
Diagnostic assessment
Serum uric acid was elevated (7.2 mg/dL) on 05 June 2019 [Figure 6].
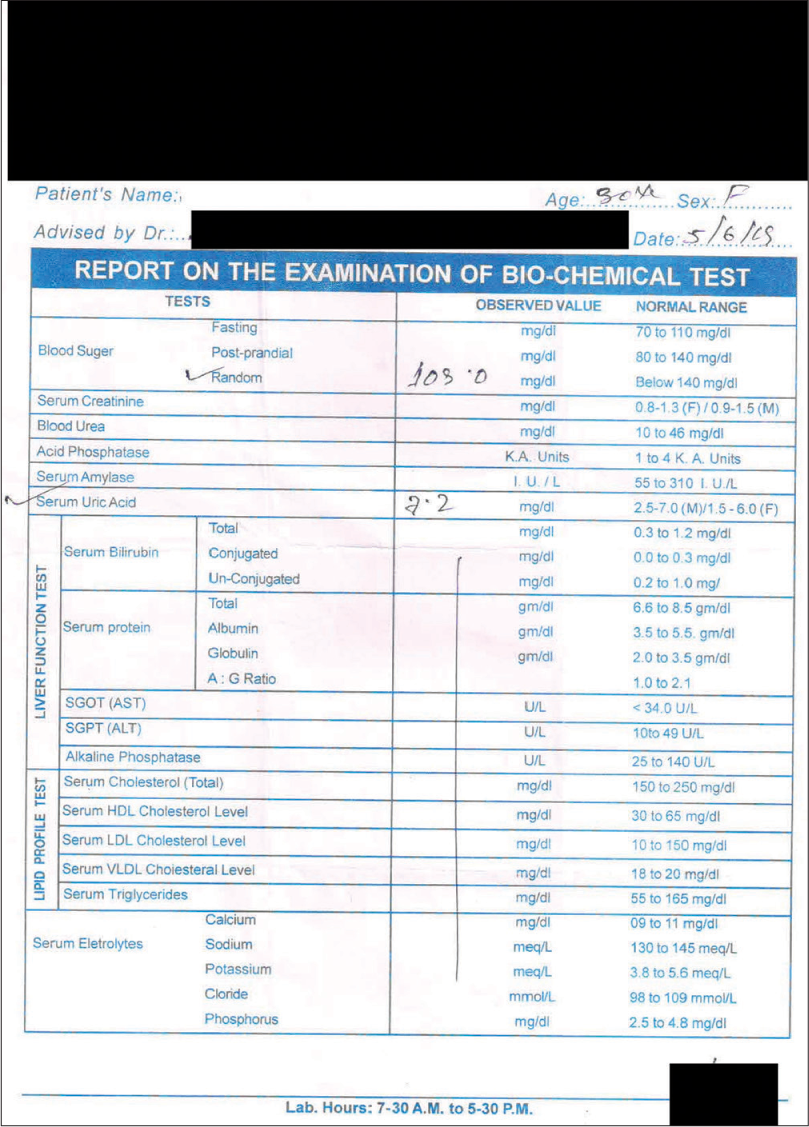
- Blood examination report of Case 2 on 05/06/2019. HDL: High-density lipoprotein, LDL: Low-density lipoprotein, VLDL: Very low-density lipoprotein, SGOT: Serum glutamic-oxaloacetic transaminase, SGPT: Serum glutamic pyruvic transaminase.
Therapeutic intervention
Repertorial analysis was done using Kent’s repertory from RADAR 10 software (Schroyens F. RADAR 10, Archibel Homoeopathic Software). The repertorisation chart is presented in Figure 7. Medicines with maximum scores were Lycopodium, Zincum metallicum, Veratrum album, Pulsatilla and Arsenic album. Considering her thermal reaction along with her physical appearance, Lycopodium was selected to begin the treatment.
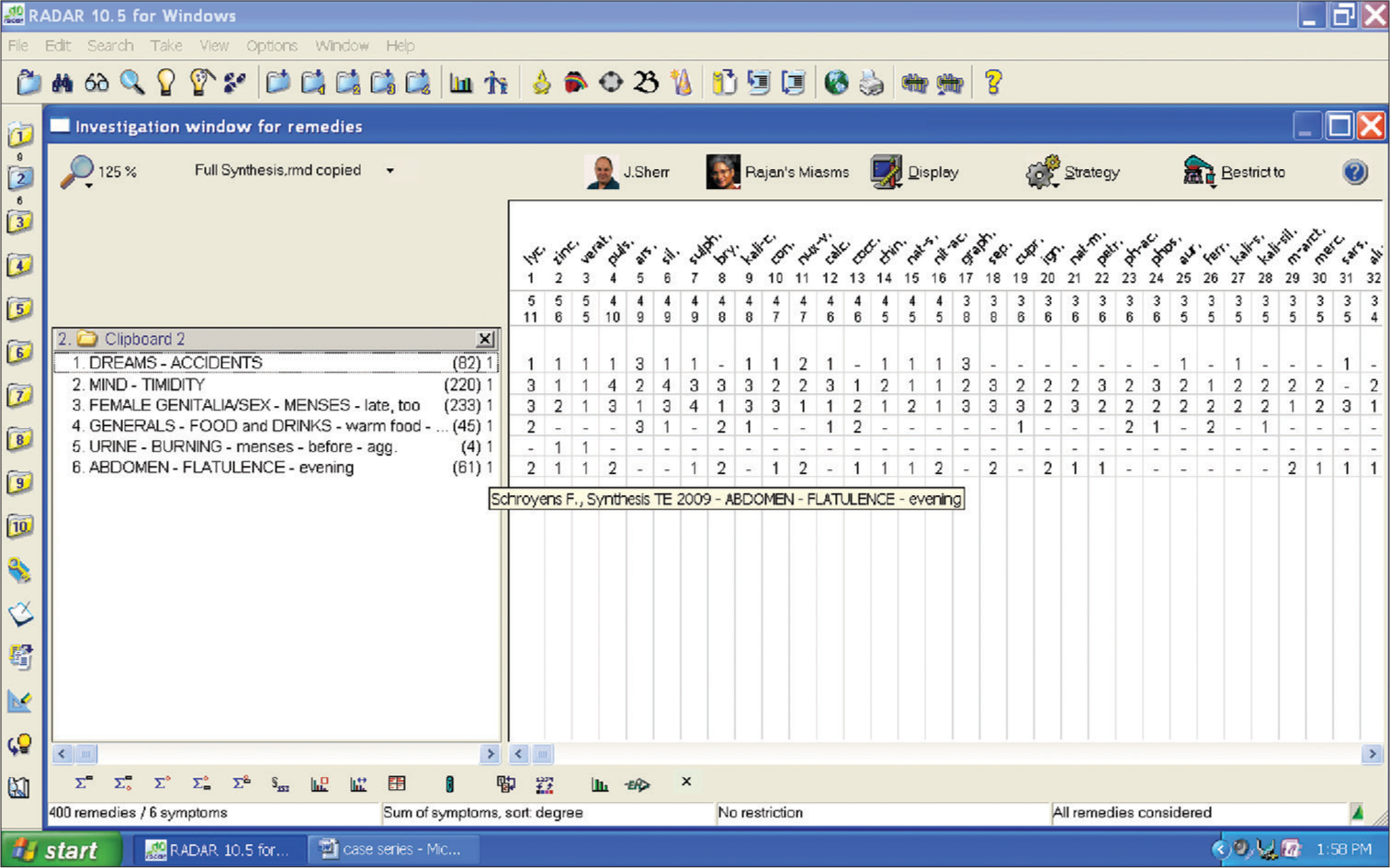
- Repertorisation chart of case no. 2.
The possible causal attribution of the treatment outcome was assessed using the modified Naranjo Criteria as proposed by the HPUS clinical data working group [Table 1]. The score obtained (10) reflects that improvement in the patient can be attributed to the homoeopathic medicine administered. MYMOP 2 score was 4.5 at the baseline and 0.25 after treatment. Follow-up [Table 3] of the patient along with reports [Figures 8-10] were assessed as per the requirement of the case.
| Date | Symptoms | Laboratory values | Prescription | MYMOP 2 Score |
|---|---|---|---|---|
| 26/06/2019 (1st visit, baseline) |
Pain in the right ankle joint. Low back pain, which radiates toward the right knee < lying on the right side, after heavy exertion > relieved by warmth. | Serum uric acid on 05/06/19 [Figure 6]: 7.2 mg/dL. |
Lycopodium 30/TDS/1 day Placebo 30/TDS/7 days |
4.5 |
| 04/07/2019 | Pain in ankle same, low back pain better, flatulence disappeared. | - | Lycopodium 200/1 dose; Placebo 30/TDS/14 days | 3.5 |
| 22/07/2019 | The pain in ankle was better, low back pain disappeared. | Serum uric acid was advised. | Placebo 30/TDS/14 days | 1.75 |
| 05/08/2019 | No further improvement in ankle pain, hence higher potency of the same medicine prescribed. | Serum uric acid on 26/07/19 [Figure 8]: 5.4 mg/dL |
Lycopodium 1M/1 dose; Placebo 30/TDS/14 days |
1.75 |
| 09/09/2019 | Ankle pain was relieved completely. | Serum uric acid was advised. | Placebo 30/TDS/14 days | 0.25 |
| 15/10/2019 | Ankle pain again started 3–4 days after eating meat. One more dose repeated. | Serum uric acid was advised. |
Lycopodium 1M/1 doses; Placebo 30/TDS/14 days |
1.75 |
| 11/11/2019 | Ankle pain disappeared. | Serum uric acid was advised. | Placebo 30/TDS/14 days | 0.25 |
| 25/11/2019 | No complaints. The patient reported to show the investigation reports. | Serum uric acid on 15/11/19 [Figure 9]: 3.97 mg/dL |
Placebo 30/TDS/14 days | 0.25 |
| 17/01/2020 | No complaints. Serum uric acid was advised for follow-up. | Serum uric acid was advised. | Placebo 30/TDS/14 days | 0.25 |
| 24/01/2020 | No complaints. The patient was much better. | Serum uric acid on 20/01/20 [Figure 10]: 3.8 mg/dL |
Placebo 30/TDS/14 days | 0.25 |
MYMOP 2: Measure yourself medical outcome profile 2
- Blood examination report of Case 2 on 26/07/2019. HDL: High-density lipoprotein, LDL: Low-density lipoprotein, VLDL: Very low-density lipoprotein, SGOT: Serum glutamicoxaloacetic transaminase, SGPT: Serum glutamic pyruvic transaminase.
- Blood examination report of case 2 on 15.11.2019.
- Blood examination report of case 2 on 20.01.2020.
Case 3
Patient information
A 62-year-old patient with a mesomorphic build, a field worker with low socioeconomic status, reported pain and swelling in both knee joints for the past three months. Pricking pains often became severe and prevented him from doing his day-to-day activities, especially in the field. The pain worsened from warmth and was better by cold application. His personal history included addiction to alcohol and smoking for ten years. The patient also complained of frequent urination with a weak stream and interrupted flow for the past two months. All his complaints aggravated during rainy damp weather, indicating a hydrogenoid constitution. His thirst and appetite were good. His thermal reaction was hot. Mentally, he was dominating his family but very obedient to his employer. His wife revealed he used to beat her very often after consuming alcohol.
Clinical findings
A general physical examination revealed a normal pulse (68 beats/min), preclinical hypertension (144/84 mm Hg) and no cyanosis or clubbing. His BMI was 23 kg/m2 (weight 68 kg, height 171 cm). His tongue was moist and clean. Mild pallor was noted. His nails were deformed with generalised roughness of skin. On examination of knee joints, there was redness and swelling, with crackles on movement. After carefully analysing the symptoms, the characteristic general and particular symptoms considered for repertorisation were dominating nature, alcohol addiction, general aggravation during rainy, damp weather, frequent urination, weak and interrupted flow of urine and joint pain > cold application.
Diagnostic assessment
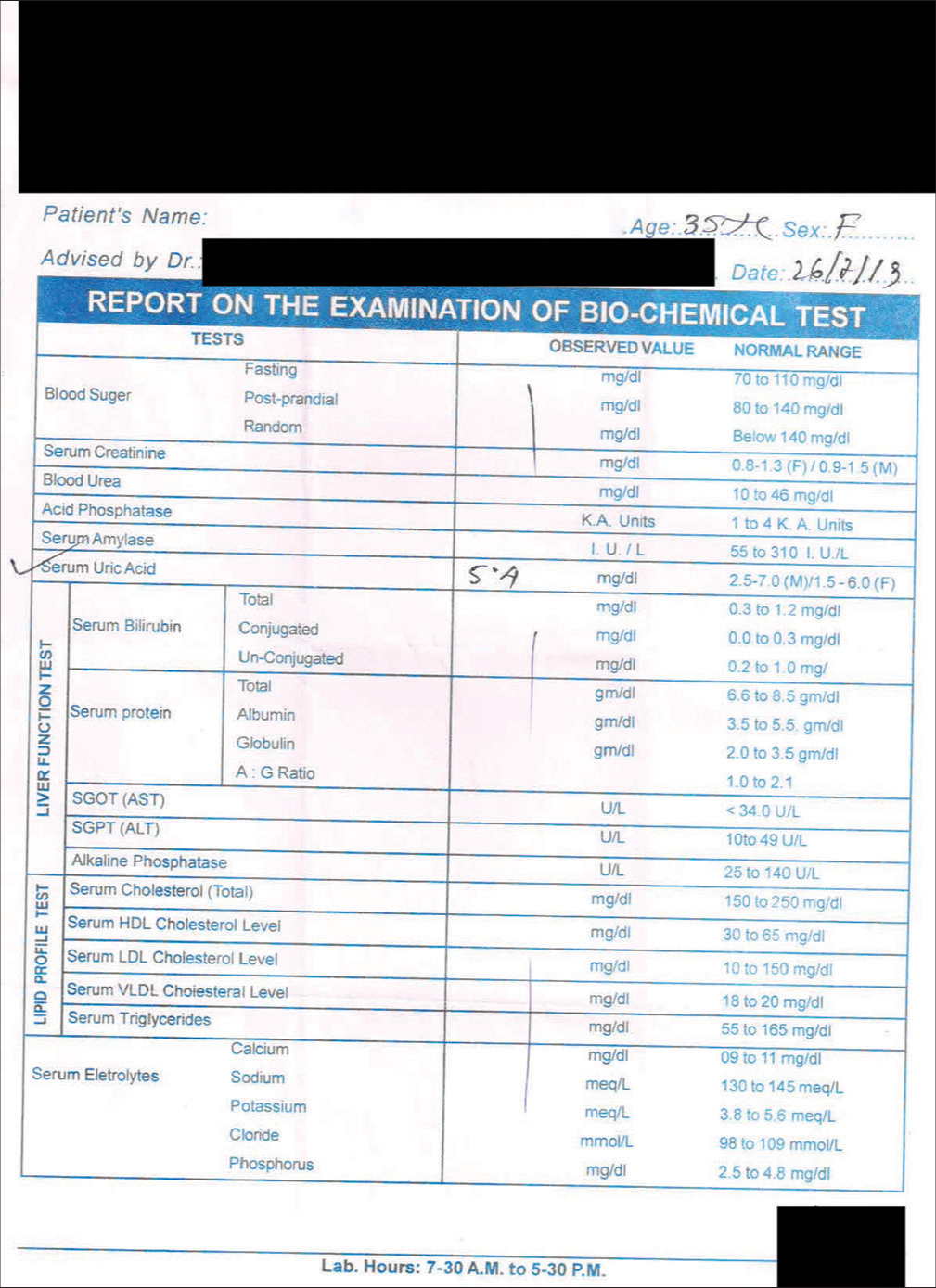
Serum uric acid was elevated (7.7 mg/dL) on 07 June 2019 [Figure 11], and post-prandial blood sugar was also slightly elevated (158 mg/dL).
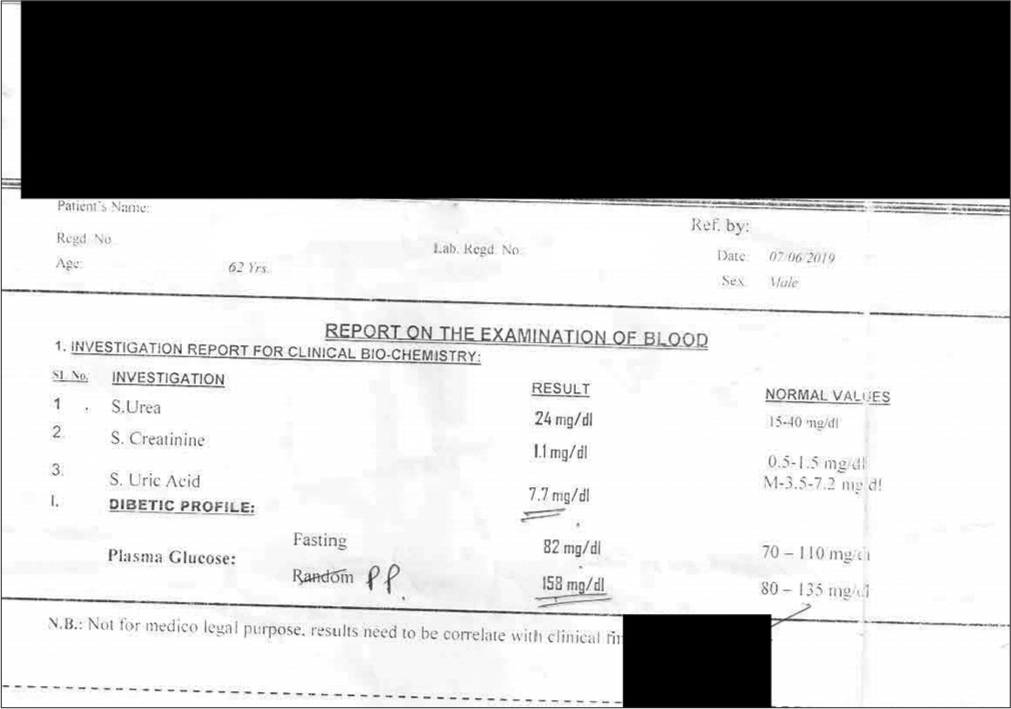
- Blood examination report of Case 3 on 07/06/2019.
Therapeutic intervention
Repertorial analysis was done using Kent repertory from RADAR 10 software (Schroyens F. RADAR 10, Archibel Homoeopathic Software). The repertorisation chart is presented in Figure 12. Medicines with maximum scores were Lycopodium, Nux vomica, Pulsatilla, Thuja and Phosphorus. Among these, only Lycopodium and Pulsatilla were hot remedies, and as the patient was domineering mentally, Lycopodium was more strongly indicated. Treatment was started with Ledum palustre based on keynote symptoms and acute totality (i.e., joint pain better by cold application), and one dose of Ledum palustre 30 was prescribed. It was followed by an intercurrent remedy and a change of prescription as per the case requirement. During treatment, significant improvement was noted in symptoms as well as serum uric acid levels. Along with treatment, dietary management was also advised.
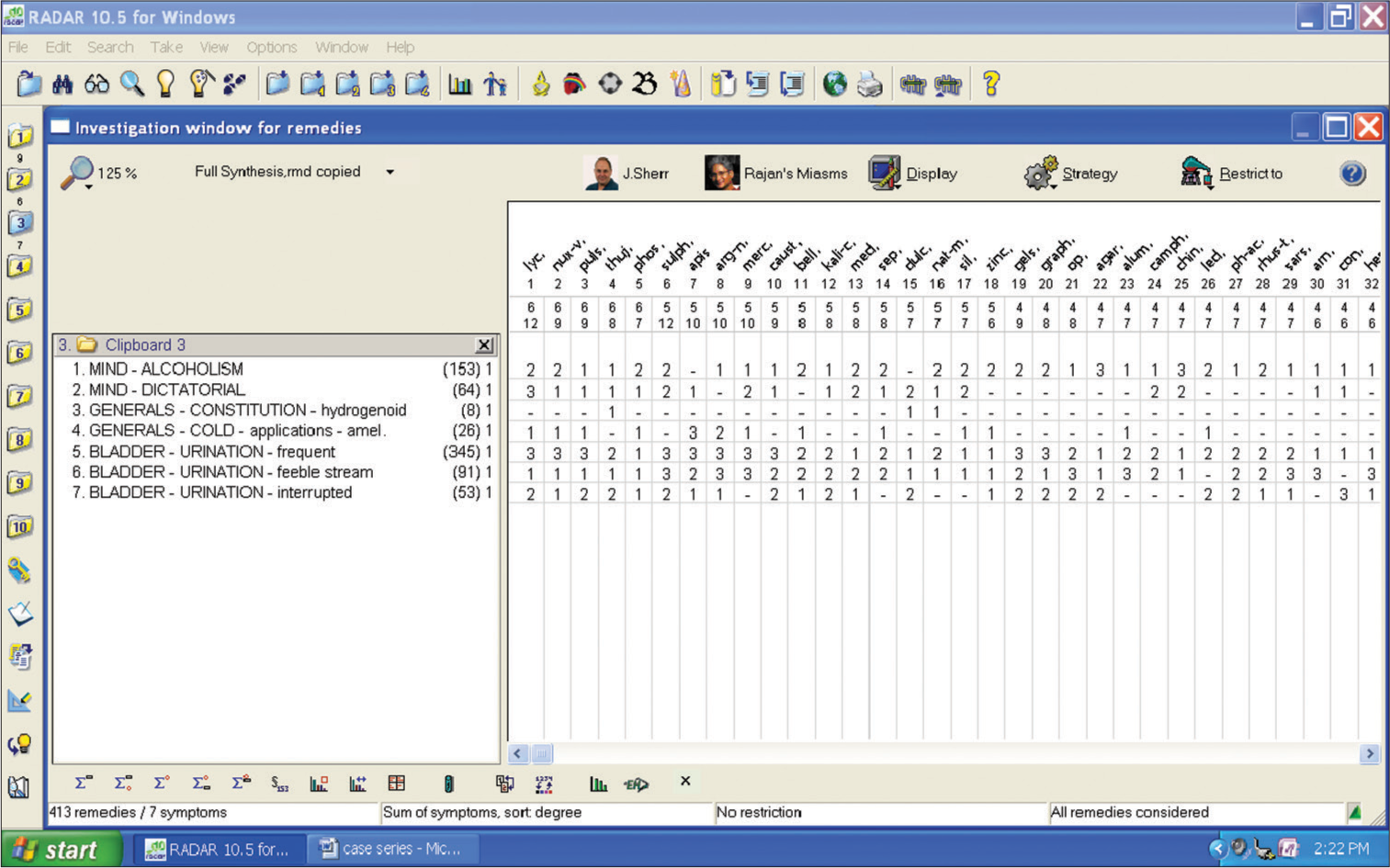
- Repertorisation chart of case no. 3.
The possible causal attribution of the treatment outcome was assessed using the modified Naranjo criteria as proposed by the HPUS clinical data working group [Table 1]. The total score obtained of nine reflects a probability that improvement in the patient can be attributed to the homoeopathic medicine administered. MYMOP 2 score was 5.3 at the baseline and 1.0 after treatment. Follow-up [Table 4] of the patient along with reports [Figures 13-15] were assessed as per the requirement of the case.
| Follow update | Indication | Laboratory values | Medicine with dose | MYMOP 2 score |
|---|---|---|---|---|
| 04/06/2019 1st visit (baseline) |
Pain and swelling of both knee joints. Pain> cold application. History of alcohol addiction |
Serum uric acid was advised. |
Ledum palustre 30/1 dose; Placebo 30/TDS/7 days |
5.3 |
| 10/06/2019 | No significant change. The potency of the same medicine was raised. | Serum uric acid: 7.7 mg/dL on 07/06/2019 [Figure 11]. |
Ledum palustre 200/1 dose; Placebo 30/TDS/14 days |
5.3 |
| 01/07/2019 | The pain was better, but there was aggravation for three days due to heavy alcohol drinking. One dose was repeated. | - | Ledum palustre 200/1 dose; Placebo 30/TDS/14 days | 5.0 |
| 19/07/2019 | The pain was slightly better. The patient complained of slight burning in urination. Due to initial relief, only placebo was prescribed. | - | Placebo 30/TDS/14 days | 4.25 |
| 27/07/2019 | Only mild relief. Considering hydrogenoid constitution and frequency of urination with weak stream and interrupted flow of urine, anti-miasmatic remedy was prescribed. | Serum uric acid was advised. | Thuja 200/1 dose; Placebo 30/TDS/14 days | 4.0 |
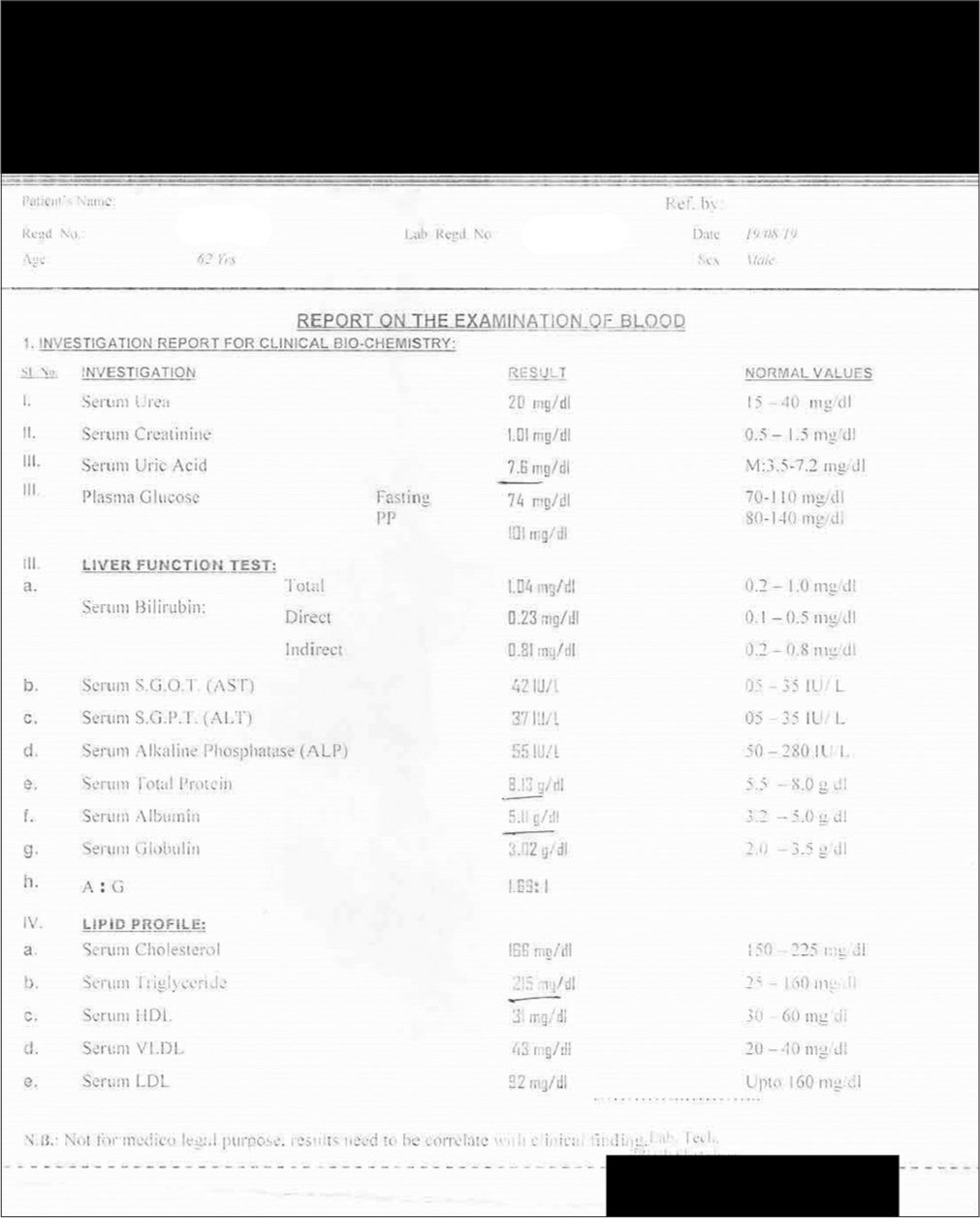
| 21/08/2019. | Pain in joints same. Burning urination relieved Much improvement in the flow of urine and frequency. Only mild relief in joint pain. Based on mental and physical generals, the constitutional remedy was prescribed. | Serum uric acid: 7.6 mg/dL on 19/08/2019 [Figure 13]. Raised serum triglycerides: 216 mg/dL | Lycopodium 200/1 dose; Placebo 30/TDS/14 days | 3.5 |
| 23/09/2019 | Much improvement in the frequency and flow of urine. Pain in joints was better. | Serum uric acid was advised. | Lycopodium 200/1 dose; Placebo 30/TDS/14 days | 2.75 |
| 27/09/2019 | Improvement in pain but not much improvement in the reduction in serum uric acid levels; hence, the potency of the same medicine was raised. | Serum uric acid: 7.5 mg/dL on 23/09/2019 [Figure 14]. Serum triglycerides: 142 mg/dL (within normal limits) |
Lycopodium 1M/1 dose; Placebo 30/TDS/14 days | 2.75 |
| 21/11/2019 | Pain in joints relieved completely. The frequency and weak flow of urine completely relieved. | Serum uric acid was advised. | Placebo 30/TDS/14 days | 1.0 |
| 27/11/2019 | The patient was much better. All complaints relieved. | Serum uric acid: 6.7 mg/dL on 25/11/2019 [Figure 15]. | Placebo 30/TDS/14 days | 1.0 |
MYMOP 2: Measure yourself medical outcome profile 2
- Blood examination report of Case 3 on 19/08/2019, HDL: High-density lipoprotein, LDL: Low-density lipoprotein, VLDL: Very low-density lipoprotein, SGOT: Serum glutamic-oxaloacetic transaminase, SGPT: Serum glutamic pyruvic transaminase.
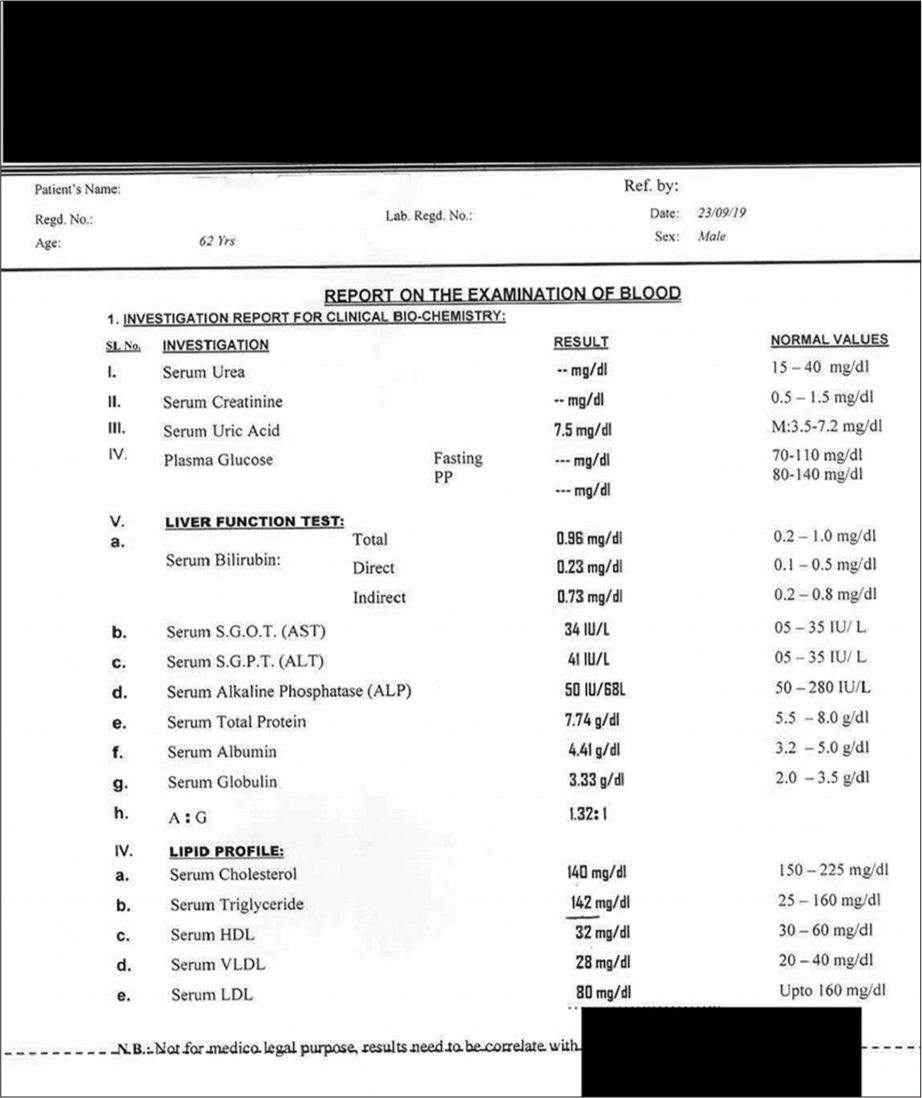
- Blood examination report of Case 3 on 23/09/2019, HDL: High-density lipoprotein, LDL: Low-density lipoprotein, VLDL: Very low-density lipoprotein, SGOT: Serum glutamic-oxaloacetic transaminase, SGPT: Serum glutamic pyruvic transaminase.
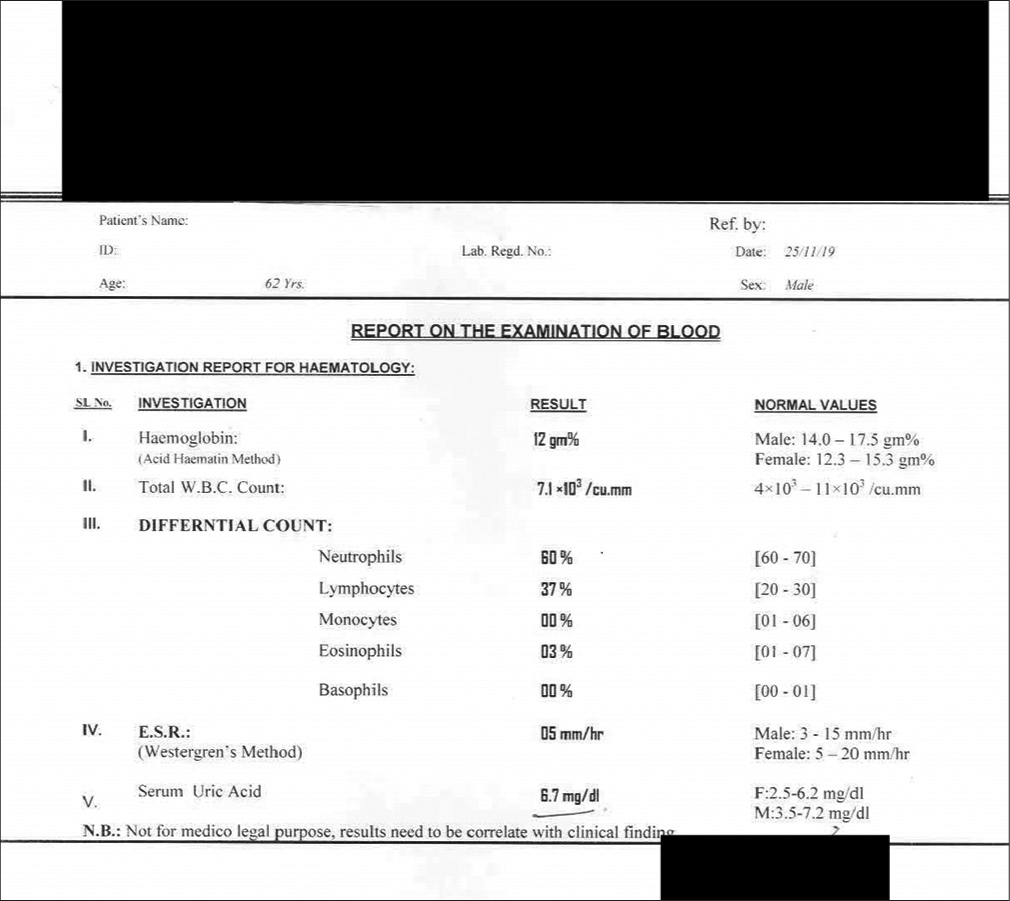
- Blood examination report of Case 3 on 25/11/2019, ESR: Erythrocyte sedimentation rate.
DISCUSSION
In all the cases, detailed case-taking was done following homoeopathic principles. The patient’s presenting complaints were assessed, along with well-marked physical generals and mental generals. Individualised homoeopathic medicines were administered after repertorisation and referred to the Materia Medica. Wherever required, intercurrent and acute medicines were also prescribed. All the patients were advised of necessary lifestyle modifications.
In case 1, the patient presented with pain in small joints along with a few gastric ailments and was diabetic and pre-hypertensive. There was an elevation of serum uric acid serum creatinine, and routine screening revealed dyslipidaemia also. The case was progressing toward metabolic syndrome. Nux vomica was given on the totality of symptoms. Intervention with homoeopathic similimum certainly prevented the progression toward other comorbidities along with improvement in other deranged biochemical parameters. The patient also benefitted from the other subjective symptoms. In this case, serum uric acid levels also decreased from 7.8 mg/dL to 5.9 mg/dL.
In case 2, a young lady aged 30 years complained of pain in the right ankle joint along with lower back pain. She was already a known case of hyperuricaemia and had been maintaining all dietary restrictions as advised but without any significant relief. Treatment was started with Lycopodium on the basis of symptom similarity. Improvement with the treatment started immediately with a marked decline in serum uric acid levels, which were maintained thereafter. Serum uric acid decreased from 7.2 mg/dL to 3.8 mg/dL after homoeopathic treatment.
In case 3, a 62-year-old field worker presented with pain and swelling of both knee joints. As there is an association between hyperuricaemia and the progression of knee osteoarthritis, as reported by Hart et al. and Al Afraj et al.,[19,20] both conditions were taken care of. Treatment was started with a keynote prescription of Ledum palustre due to acute presentation. It was followed by Thuja as anti-miasmatic and finally with Lycopodium as constitutional treatment. His serum uric acid levels decreased from 7.7 mg/dL to 6.7 mg/dL after treatment.
In Cases 1 and 2, the patients responded very well to the constitutional medicine, but in Case 3, the patient presented with acute symptoms;[19,20] treatment was therefore initiated with an acute remedy based on the keynote symptoms. However, the patient was only palliated with a recurrence of complaints. Hence, one dose of deeper-acting anti-miasmatic medicine was administered to remove the miasmatic block, considering his predominant symptoms like frequent urination with weak stream interrupted flow, probably due to benign prostatic hyperplasia, considering his age. He used to beat his wife very often but was very obedient to his employer and had a dominating nature, which is also observed in the psychotic mind. It was then followed by constitutional treatment.
Improvement in cases was assessed clinically based on the changes in signs and symptoms. MYMOP2 scores were recorded in each follow-up for measuring clinical change associated with the course of homoeopathic treatment. The modified Naranjo criteria[21] were used for analysing any adverse effects and validating the symptoms after the medicine had acted. The modified Naranjo criteria are a valid tool for assessing the likelihood of a causal relationship between homoeopathic intervention and clinical outcome. Serum uric acid levels were also measured periodically.
Serum uric acid levels decreased gradually until they normalised with continued homoeopathic treatment, along with significant clinical improvement in all the abovementioned cases. MYMOP 2 scores also decreased gradually from baseline till the end of treatment with homoeopathic medicines. In this case series, each patient had a reduced score at every follow-up, which further decreased significantly by the end of treatment [Table 5]. In all the cases, the total score of the outcome as per the modified Naranjo criteria score after treatment was nine or more, which is close to the total score of 13 and explicitly shows the positive causal attribution of the individualised homoeopathic medicine prescribed. In all the cases, the serum uric acid levels improved, along with other biochemical parameters.
| Cases | Pre-intervention uric acid level |
Post-intervention uric acid level |
|---|---|---|
| Case 1 | 7.8 mg/dL | 5.9 mg/dL |
| Case 2 | 7.2 mg/dL | 3.8 mg/dL |
| Case 3 | 7.7 mg/dL | 6.7 mg/dL |
All the cases had hyperuricaemia, but the manifestations were different. Hyperuricaemia, although not a disease in itself, can give rise to several diseases if not addressed in a timely manner. In all the cases, after considering the totality of symptoms, the indicated medicine was prescribed, which started the reversal of derangements with subjective as well as objective improvement reflected in form lab reports, thereby depicting the restoration of derangement in purine metabolism. Hyperuricaemia is an important mediator of gout and is associated with metabolic syndrome, diabetes, hypertension and kidney and cardiovascular diseases.[22] One case was diabetic, and two had pre-hypertension. In one study by Barbieri et al., uric acid levels are significantly higher in men,[23] which corroborates with our case series where two out of three cases were men. Another study by Deep and Kumar showed a significant role of homoeopathic medicines in the management of hyperuricaemia in gout.[15] Our findings concur with the results of this study and our earlier published case report.[9] The prescribing method used in one of our cases was similar to that used in a case report by Bala and Shrivastava, where a cure was achieved by multiple medicines administered periodically, changed from time to time as per the requirement of the case.[8] In this study, out of four cases in three cases, Lycopodium was the most commonly used polychrest medicine for uric acid diathesis in three out of four cases.
In the 4th aphorism of Organon of medicine, Hahnemann describes preventive healthcare, which aims to protect, promote and maintain health and well-being by preventing disease in the first place. Timely intervention with proper homoeopathic treatment can prevent further progress and probably other comorbidities. This case series further adds to the evidence of the effectiveness of homoeopathy throughout the disease, that is, preclinical conditions to fully developed disease.
However, the authors accept that the possibility of spontaneous decline could not be ruled out completely. This case series may be a small contribution toward shedding some light on the scope of homoeopathy in this less unexplored area. However, randomised and controlled studies with long-term follow-up and larger sample sizes are required to generate stronger evidence.
CONCLUSION
The holistic approach adopted during homoeopathic treatment has the potential to not only provide symptomatic relief but also prevent several other disease conditions. Homoeopathy is also safe and does not cause drug dependency. In this case series, three cases of hyperuricaemia were effectively treated with homoeopathic remedies. There were no reports of adverse effects. In the future, randomised controlled trials with larger sample sizes are suggested to establish the efficacy of homoeopathic constitutional remedies in the treatment of hyperuricaemia.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Davidson’s principles and practice of medicine (23rd ed). UK: Elsevier; 2018. p. :1360.
- [Google Scholar]
- Hyperuricemia prevalence in Indian subjects with underlying comorbidities of hypertension and/or type 2 diabetes: A retrospective study from subjects attending hyperuricemia screening camps. Int J Res Med Sci. 2020;8:794-800.
- [CrossRef] [Google Scholar]
- Hyperuricemia and coronary heart disease: A systematic review and meta-analysis. Arthritis Care Res (Hoboken). 2010;62:170-80.
- [CrossRef] [PubMed] [Google Scholar]
- Is hyperuricemia an independent risk factor for new-onset chronic kidney disease?: A systematic review and meta-analysis based on observational cohort studies. BMC Nephrol. 2014;15:122.
- [CrossRef] [PubMed] [Google Scholar]
- Therapeutic strategies for the treatment of chronic hyperuricemia: An evidence-based update. Medicina (Kaunas). 2021;57:58.
- [CrossRef] [PubMed] [Google Scholar]
- A case of gout treated with Homoeopathic constitutional remedy. Int J Homoeopath Sci. 2020;4:365-8.
- [CrossRef] [Google Scholar]
- case report on hyperuricemia presenting as one-sided disease. Homœopathic Links. 2019;32:105-11.
- [CrossRef] [Google Scholar]
- A case report of hyperuricaemia with nephrolithiasis treated with homoeopathy. Indian J Res Homoeopathy. 2021;15:147-54.
- [CrossRef] [Google Scholar]
- Individualised homeopathic medicines and Urtica urens mother tincture in treatment of hyperuricemia: An open, randomised, pragmatic, pilot trial. J Complement Integr Med. 2020;18:599-608.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of Ocimum sanctum and Ledum palustre on serum uric acid level in patients suffering from gouty arthritis and hyperuricemia. Bull Chem Soc Ethiop. 2013;27:469-73.
- [CrossRef] [Google Scholar]
- Individualised homeopathy as an adjunct in the treatment of gout-a randomised placebo controlled trial. Allg Hom Ztg. 2017;262:2-76.
- [CrossRef] [Google Scholar]
- An open-label prospective observational trial for assessing the effect of homoeopathic medicines in patients suffering from gout. Indian J Res Homoeopathy. 2019;13:236-43.
- [CrossRef] [Google Scholar]
- Homoeopathic management of hyperuricemia in primary gout: A randomised single blind placebo controlled study. Int J Homoeopath Sci. 2020;4:73-7.
- [CrossRef] [Google Scholar]
- The homoeopathic simillimum treatment of acute arthritis in primary gout in terms of the illness intrusiveness scale, blood uric acid levels using the uricase conversion method as well as the acupulse homeostat machine [dissertation] 2001. Durban: Technikon Natal; Available from: https://hdl.handle.net/10321/2069 [Last accessed on 2023 Mar 21]
- [Google Scholar]
- Individualised homeopathic medicines in treatment of hyperuricemia: Evaluation by double-blind, randomised, placebo-controlled trial. Homeopathy. 2023;112:85-96.
- [CrossRef] [PubMed] [Google Scholar]
- Assessing patient outcomes in acute exacerbations of chronic bronchitis: The measure your medical outcome profile (MYMOP), medical outcomes study 6-item general health survey (MOS-6A) and EuroQol (EQ-5D) Qual Life Res. 2000;9:521-7.
- [CrossRef] [Google Scholar]
- Association between metabolic factors and knee osteoarthritis in women: The Chingford Study. J Rheumatol. 1995;22:1118-23.
- [Google Scholar]
- Evaluation of the modified Naranjo criteria for assessing causal attribution of clinical outcome to homeopathic intervention as presented in case reports. Homeopathy. 2020;109:191-7.
- [CrossRef] [PubMed] [Google Scholar]
- Hyperuricemia, the kidneys, and the spectrum of associated diseases: A narrative review. Curr Med Res Opin. 2016;32:1863-9.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of sex on uric acid levels and its relationship with the extent of coronary artery disease: A single-center study. Atherosclerosis. 2015;241:241-8.
- [CrossRef] [PubMed] [Google Scholar]




