
Translate this page into:
Studying the evolution of miasm in autism spectrum disorders: A case series
*Corresponding author: Sunita Bhanudas Nikumbh, Department of Psychiatry, Dr. M. L. Dhawale Memorial Homoeopathic Institute, Palghar - 401 404, Maharashtra, India. sunita.nikumbh@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nikumbh SB. Studying the evolution of miasm in autism spectrum disorders: A case series. J Intgr Stand Homoeopathy 2020;3(2):43-50.
Abstract
Objectives:
Autism spectrum disorder (ASD), a neurodevelopmental disorder, is one of the several developmental disorders observed in children. The current prevalence of ASD among those under 18 years of age is 0.09 and 0.11 in an urban and rural area, respectively. Being a developmental disorder, it starts showing signs in the first 3 years of life and is present for the rest of the individual’s life. Studies have identified genetic predominance and a disturbed mental state in the mother during pregnancy in the genesis of disease. Modern medicinal interventions target only some specific and uncontrolled behaviours in ASD children; hence, the management is focused mainly on self-sustenance with integrated care with the help of ancillary therapies. Homoeopathically, these factors carry considerable importance as they contribute to the fundamental or miasmatic load, based on which the totality is formulated to select homeopathic simillimum. This paper studies the miasm in ASD cases treated in the Child Psychiatry OPD at Dr. M. L. Dhawale Memorial Homoeopathic Institute, Palghar (2015–2018) by studying miasmatic load in detail.
Materials and Methods:
ASD cases diagnosed according to ICD-10 criteria were studied in detail with evolutionary data collected from parents in terms of current complaints and illnesses (past, personal and family) in both families and were analysed for miasmatic load. The fundamental and dominant miasm derived from the disease expressions and history of family illnesses. Homoeopathic simillimum selected based on the predominant miasm/s along with the totality erected as per the available characteristic expressions in the cases.
Results:
Administration of simillimum healed the patient at the constitutional and miasmatic level and resulted insignificant improvement in the characteristic expressions in the patients. Timely identification and intervention yield a quicker response.
Conclusion:
Selecting homoeopathic remedies that cover the miasmatic background yields good results in children with ASD.
Keywords
Autism spectrum disorder
Miasm
Evolution of miasms

INTRODUCTION
Autism spectrum disorder (ASD) is characterised by persistent deficits in social communication, social interaction and non-verbal communication along with repetitive or meaningless gestures as well as marked and sustained impairment in social relationships. There is almost a congenital ‘inability to relate’ to people in the usual ways. Unusual responses to the environment include stereotyped motor mannerisms and resistance to change. Pronoun reversal and a tendency to echo language also occur.[1] The current prevalence of ASD in the 1–18 years age group in India is 0.09 in urban areas and 0.11 in the rural regions.[2]
The definite cause of ASD is unknown. Autism runs in families; genetics plays a significant role.[3] Some susceptible genes responsible for its pathogenesis have been identified recently.[4] Environmental factors also play a major role. Illnesses during pregnancy and after delivery are significant in the genesis of ASD. Psychodynamic theories have proposed that the mother’s mental state during pregnancy is significant for establishing the mother-child bond; disruption or non-development of the bond hampers the child’s development.[5]
The intensity of these factors decides the characteristic presentation of disturbances or changes occurring during paediatric development. Evolution of disease that is, onset, pace and progress is decided by these factors as well.[5] Since ASD is a neurodevelopmental disorder, neurological disturbances affect the child’s overall development. Impairment occurs at the developmental, intellectual, cognitive and emotional levels. In general, symptoms represent an individual’s reaction to the inherited predisposition as seen in susceptible constitution and disturb the functioning of the affected organs and systems, which are affected by the environmental changes.
Changes in brain structure with changes in neurotransmitters are responsible for physical, physiological and psychological growth of the individual from the embryonic state. The amygdala and limbic systems are the main structures disturbed in ASD; they govern perception of emotions and emotional responses. Pathological changes in these structures result in unresponsiveness to stimuli; the child appears deaf, mute and apathetic to their environment.
Emotional perception and learning do not occur as the child cannot register the visual memories of objects/humans/ substances around and store or retrieve. This gives a feeling of the child being unresponsive to the surroundings. Hyperresponses at the behavioural and emotional levels occur because of increased convexity of mirror neurons; this results in restlessness, meaningless gestures and echolalia. The child fails to interpret biological movements and cannot understand how to relieve itself. Use of nonverbal gestures to indicate the urge to pass stool/urine is not developed in the child.[6]
Multiple factors affect ASD genesis; it is difficult to define the role of every structure and factor.[5] Hence, deriving miasm in ASD is a challenge for every homoeopathic physician. We will demonstrate the process with few cases treated successfully with homoeopathy.
Psychiatry employs an integrated approach, focusing on making the child independent and self-sufficient through strengthening the neuromuscular coordination and networking rather than addressing the pathology itself. Hence, all ancillary therapies are geared to improving the skills required for daily living, social reciprocation and communication. Medicinal intervention targets some specific and uncontrolled behaviour in ASD children.[6] Every individual is born with some hereditary features and some susceptible predisposition. Each individual has characteristic expressions in three basic levels: Physical, emotional and intellectual. These three constituents strongly influence each other. Individual expressions of disease are largely determined by the predisposition, which decides the onset, course, pace and progress of disease; the genetic structure functions accordingly. Every constitution has the propensity to develop illness – the weakest body system/organ/tissues/ cell and the functions that fail to maintain harmony are indicated through relevant symptomatology.[7]
Homoeopathic concepts of causation and its relationship with miasms
Dr. Hahnemann used the term miasm with two perspectives: One is the ‘pollution’ that ‘causes the disease’ and another is the ‘noxious influence or atmosphere’ that influences the disease process. Dr. Hahnemann grouped miasm into Psora, Sycosis and Syphilis. Tubercular is the fourth miasm, a combination of pseudo-Psora with Sycosis or Syphilis; it was defined by Close and Allen.[8] Loading from heredity along with the predisposition determines the miasmatic evolution in disease [Figure 1].
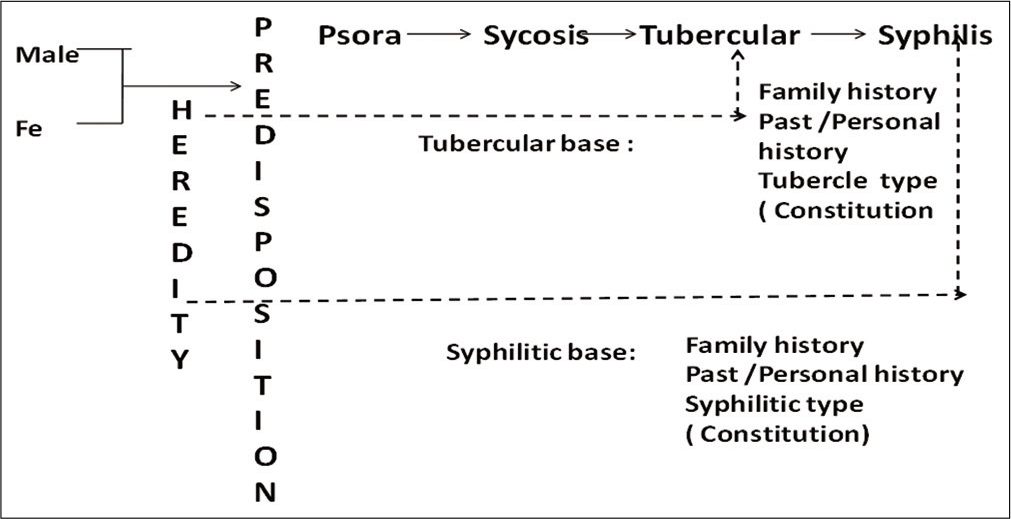
- Evolution of miasm.
- Symposium Volume, Area B. p. B41-8. Reprint with permission from Dr. M.L. Dhawale Memorial Trust; Mumbai
MATERIALS AND METHODS
Children reporting with developmental issues were evaluated based on expressions or symptomatology; diagnosis was confirmed using the ICD-10 criteria and Childhood Autism Rating Scale (CARS) or Indian Scale for Autism Assessment (ISAA). Homoeopathic data were gathered by collecting information from the parents and recorded with the Standardized Case Record©.[8,9] The data were analysed as follows: Disease onset, disease pace (past/personal/family), clinical presentation with characteristic expressions, presence of comorbidity, dispositional qualities, maternal obstetric history and mental state during pregnancy and after delivery.
Responses to intervention were evaluated with the help of follow-up criteria, which were prepared per the presenting symptoms. Release of intercurrent remedy was decided after studying the remedy response.
Descriptive cases
Case report 1
Master PSM: A 3-year-old boy with complaints of restlessness, constantly jumping, self-hurting+++ behaviour, hitting his head or slapping himself loudly without any obvious pain, constant thumb sucking and monosyllabic speech. He sniffs all foods before eating. Sleep is the only time he is quiet.
Physical generals
Lean, thin child. Intense cravings Egg+++, Chicken++, Chocolate++, Fish++, Sour++ and prefer warm food or drinks++.
History
Two episodes of eruptive fever (?measles); one at 8 months and at 1 ½ years. He was born with a convergent squint and was operated for esotropia, amblyopia and myopia.
Mother’s obstetric history
First pregnancy: Hepatitis, typhoid and malaria during the first pregnancy, delivered a stillborn. The patient is the second child; pregnancy was uneventful.
Mother’s mental state during pregnancy: Anxiety regarding delivery.
Developmental milestones: All normal except speech.
Investigations: EEG January 24, 2012: Sleep record abnormal in view of epileptiform activity present over bilateral centrotemporal region independently.
MRI December 23, 2011: Chronic sequelae of perinatal hypoxic ischemic insult with bilateral slightly atrophy of brainstem.
Because of hyperactivity, the child could not undergo psychometric tests. Behavioural expressions were suggestive of ASD with epilepsy per ICD-10.
Family history
Paternal grandfather died of pulmonary tuberculosis
Paternal grandmother: Hypertension with complications, sudden death
Maternal grandfather: Myocardial infarction (MI) causing sudden death.
Case analysis
The fundamental (family) load is heavily syphilitic, especially from mother whose tubercular miasm in terms of infections caused still birth (syphilitic miasm).
Before the patient’s birth, the deaths in the family were due to pulmonary Koch’s and sudden deaths because of hypertension and MI. This indicates tubercular-syphilitic miasm in the family. A still birth is another example of syphilitic miasm. The multiple tubercular infections in the mother during the first pregnancy have increased the effect of miasm on the susceptible genes. The child was born with a heavy fundamental miasmatic load.
The history of eruptive fever twice in a short time is characteristic of dominant tubercular miasm. The history of squint (reduced tone of eye muscles) and delayed milestones indicate sycotic miasm.
Tubercular-syphilitic expressions are seen in the form of epileptic foci in brain, incessant hyperactivity, hurting behaviour and characteristic cravings. Hence, the dominant miasm in this case is tubercular. [Table 1] shows the repertorial syndrome and remedial coverage.
| Repertorial syndrome | |
|---|---|
| Constantly jumping | Cravings: |
| Self-hurting behaviour | Egg+++, |
| Restlessness | Chicken++, Chocolate++, |
| Habit of sniffing food before eating++ | Fish++, |
| Sour++, | |
| Warm food or drinks++ |
Remedies: Calc Carb 6/9, Lyco 6/9, Tub 7/8 Medo 6/8 Phos 5/8, Tarentula 4/4
Final remedy with differentiation: Constant jumping and self-hurting behaviour were the main symptoms of this case, which were covered by Tarentula Hisp. and Tuberculinum bovinum, respectively. All the physical symptoms were covered by Tuberculinum alone. In this case, remedies such as Calc Carb and[10] Lycopodium[11] cover all the physical general and therefore have a higher coverage in the reportorial result, but lesser coverage in characteristics symptoms of the case such as constant jumping and self-hurting behaviour. These two symptoms are mainly by covered by Tarentula Hisp.[12,13] and Tuberculinum;[14] these were differentiated. In Tuberculinum, the child is independent and restless as he wants to explore new things, leading to changeability. He becomes impulsive and destructive, especially when he is frustrated due to lack of change. In Tarentula, the child is extremely restless because of boundless energy; to channelise that energy, he is compelled to be busy and has constant desire to jump. He appears impatient or hurried. There is constant movements of hands and legs but lacks control. Constant motion aggravated his complaints. Tuberculinum was considered.
Remedy selected: Tuberculinum bovinum was selected based on total correspondence at the mental, physical and miasmatic levels.
Potency and repetition: Tuberculinum bovinum 1 M, 1 dose weekly was continued for 2–3 weeks; later, 3 doses once a fortnight.
Follow-up result: The first change seen was reduction in his self-hurting behaviour over 6–8 months; the hyperactivity and restlessness also reduced. Sniffing food reduced over 15 months.
Case report 2
Master SKK: A 4-year-old male child was brought with the complaints of regression in achieved developmental stages. He had stopped using words already learnt and was currently monosyllablic+++ with meaningless, muttering, irrelevant talk+++, restlessness++, hyperactivity+++ and constant jumping+++ from high places/windows+++ with no fear of getting hurt+++. No control over bowel and bladder, untrainable. Spitting+++, no eye contact with anyone.
Physical generals
Sweats profusely on scalp+++ only at night. Hunger intolerable; gets angry immediately. Cravings: tea+++, cold drinks++, fried++, salty things++sweet++ and warm drinks++
Observations in OPD: Whenever the child gets irritated, music played on the cell phone, helps to calm him.
History
Epilepsy started at 3 years after fall on head.
Mother’s obstetric history
The first pregnancy occurred after the husband was treated for oligospermia. That child died from asphyxia during delivery. Thereafter, the mother could not conceive for 3–4 years.
Mother’s mental state during pregnancy: She felt lonely as no one was around to look after her; husband was at work. She was anxious about her baby’s health of child.
Developmental Milestones: Normal until regression started.
Investigations: EEG (12 February 2017): Epileptogenic focus in the right posterior head region with secondary bilateral synchrony.
MRI brain 12 February 2017: Small infarct in white matter of subcortical in parietal region.
ISAA score 79, mild autistic features.
Family history
Father: Diabetes mellitus, hypertension and chronic kidney disease. Mother: Gallstones underwent cholecystectomy.
Elder sister: Typhoid.
Paternal and maternal grandparents: No significant history.
Case analysis
The child was born in a tense family environment. Due to the husband’s infertility and after death of the first child, the mother was anxious throughout this pregnancy. The father’s diagnosis and mother’s cholecystitis, anxiety and inability to conceive indicate sycotic miasmatic load. Family history indicates syco2+-tubercular2+miasm. Regression in achieved milestones indicates syphilitic miasms. Overall, the dominant miasm is tubercular.
Final remedy with differentiation
[Table 2] shows the repertorial syndrome and remedial coverage. All miasmatic remedies came up in repertorisation. All remedies cover restlessness, but the intensity is less. The core of this case is in the qualified mental expressions of restlessness and music ameliorates, which are covered by Tarentula more than Tub or Carcinosin.[15] Tuberculinum shows significant changeability of symptoms with great emaciation, which was absent in this case. Stramonium covers painlessness and fearlessness with some physical generals, but does not cover the main ameliorating modality.[16] Carcinosin has sensitivity toward music but not as intense as Tarentula. All cravings except tea are covered by Tarentula; other remedies show in consistent coverage.
| Repertorial syndrome | |
|---|---|
| 1. Music ameliorates | Cravings: |
| 2. Constant jumping from high places+++ | 1. Tea+++ |
| 3. No fear of getting hurt+++ | 2. Cold drinks++ |
| 4. Spitting saliva around+++ | 3. Fried++ |
| 5. Intolerable hunger | 4. Salty things++ |
| 6. No bowel and bladder control children in | 5. Sweet++ |
| 7. Sweats on scalp+++at night |
Remedies: Tarentula 9/12, Tub bov8/11, Carcinosin 7/10, Stramonium 7/9
Remedy selected: Tarantula Hisp. selected on the above basis.
Potency and repetition: 200 C 1 dose repeated every week and then increased to daily. Child required Tuberculinum bovinum as an intercurrent whenever progress slowed. Three/four doses of antimiasmatic were required. After almost 1 year of treatment, the potency of Tarentula was increased to 1 M infrequently (1 dose weekly).
Follow-up result: Symptoms of hyperactivity, restlessness and spitting started reducing within 3–4 months. After 6 months, the speech progressed from monosyllabic to few words to small sentences. Hyperactivity and restlessness reduced considerably; at 1 ½ years, the child can attend school and performs well.
Case report 3
Master SSA: A 6-year-old male child with complaints of making meaningless sounds+++ since the age of 1 year, unclear monosyllabic speech, poor socialisation+++, hides under the table+++ when meets people but hyperactive+++ when left alone. Bangs hand on the table++ whenever angry. Uses certain gestures for communication. He has a voracious appetite and uncontrollable hunger. He is fearful and sensitive to noise; he will start weeping→ crying→screaming when in public or crowd.
Recurrent upper respiratory tract infections due to changes in weather, winter season.
Physical generals
Craving: Chocolates+++, chicken+++, fish+++, cold drinks+++, ice cream+++ Aversion: Sour items3+like curd++
Strong sensitivity to odours+++, loud noise and thunder+++
History
Medical history: Nothing significant.
Mother’s obstetric history: Caesarean section; umbilical cord was around the neck.
Post-delivery: Neonate – physiological jaundice, unable to suckle.
Mother’s mental state during pregnancy: This was the first pregnancy, low mood and anxiety as husband was away from home. She had some conflicts with mother-in-law who had come to stay with her in the pre- and post-delivery period.
Developmental landmarks and problems: Child was unable to suck and took long time to learn. He took 3–4 years to learn to chew solid food. Except speech, all milestones were normal.
Family history
Father: Hypothyroidism
Paternal grandfather: Diabetes mellitus and hypertension
Paternal grandmother: Hypothyroidism diabetes mellitus
Maternal grandmother: Diabetes mellitus.
Life space
Parents are well qualified and educated. Mother shared her observations: He is fond of cleanliness+++ since age of 1, perfectionist+++ about his things. He will wear only neat and properly ironed clothes. Has strong smell sensitivity, wants the washroom cleaned before he uses it. He likes travelling+++, especially beaches and playing with sand, makes letters. He has marked fear of injection sand dark. He needs at least one parent with him when sleeping.
Investigations
CARS: 33, indicating mild ASD.
Case analysis
The mother’s mental state was disturbed during pregnancy; she longed for her husband, but had to put up with her mother-in-law instead. The child was delivered through LSCS due to slow progress of labour, indicating sycotic miasm.
Both sides of family show diabetes, hypertension and hypothyroidism, indicating syco+++-tubercular++load.
The child’s development is slow, indicated by inability to suckle and to chew solid food. This signifies poor muscle development, indicating strong sycotic miasm+++.
Final remedy with differentiation
[Table 3] shows the repertorial syndrome and remedial coverage. All the qualified mental symptoms are covered by phosphorus, except developmental slowness at mental and physical level. Calcarea[17] covers developmental issues. Calcarea group children are born with indolence at the physical level, have difficulty in suckling and are sluggish and obstinate with hypersensitive mind with lot of desires. Therefore, Calc Phos,[18] a polycrest and anti-miasmatic remedy, was selected based on the symptoms of slowness, specific fears, travelling desire and certain physical general symptoms. Carcinosin does not cover sensitivity to odours in repertorisation, but the Materia Medica mentions it. The Carcinosin child shows slow mental development, but no physical disturbance. The child is fastidious, precautious, perfectionist, restless, likes to travel, has sensitivity to music and reprimands. Apart from perfectionism, fears and love for travelling, Carcinosin did not cover any symptoms.
| Repertorial syndrome | |
|---|---|
| Strong sensitivity to odour+++ | Cr Chicken+++ |
| Perfectionism+++children in | Chocolate+++ |
| Fears: Thunderstorm+++ | Cold drink+++ |
| Fear dark+++ | Ice cream+++ |
| Desire for travelling++ | Aversion –Curd++ |
| Sou++ |
Remedies: Phos 19/9, Lyco 13/9, Carc 11/8, Cal.Carb10/7, Nat. Mur 10/7, Sil 6/6
Remedy selected: Calcarea Phos, a multi-miasmatic remedy with a strong Tubercular coverage.
Potency and repetition: Treatment was started with Calcarea Phos 200 C 1 dose weekly, subsequently increased to 3 doses weekly.
Follow-up result: Within 4 weeks, the meaningless sounds reduced and speech improved from monosyllabic to sentences. Within 6–8 months, the fears and restlessness reduced considerably.
Case report 4
Master PCP: A 7-year-old girl with gradually progressive poor communication+++ since the age of 3 years. She repeats sentences or questions when spoken to. She pays less attention in class, mechanically following the instructions and displays noise sensitivity+++.
She has had sessions with a developmental paediatrician, occupational therapist and speech therapist, with no result.
She has recurrent upper respiratory complaints that are intense during winter.
Physical generals
Craving: Cold drinks+++, ice cream+++, sweets+++, pica++, oranges++, cakes++, milk+++; milk causes diarrhoea.
Medical History: Nothing specific.
Mother’s mental state during pregnancy: Nothing significant, although it was unplanned.
Developmental Milestones: All normal, except speech, which started at 1 ½ years of age. No bowel/bladder control yet.
Investigations: 1 December 2018.
Vineland Social Maturity Scale (VSMS): 80 (below average).
ISAA score 82, suggesting mild autistic features.
Family History
Paternal grandmother: Hypertension.
Maternal grandfather: Diabetes mellitus.
Life space
As the only girl child, she is pampered. Mother is short-tempered (similar to the child), while father has a compromising nature. Parents described her as moody. If contradicted, she gets angry and expresses anger by clenching her teeth.
At school, she is reserved and averse to touch and company.
Case analysis
No significant issues around pregnancy and post-delivery. Family history shows sycotic++ load. No developmental issues. Physical generals are Tubercular++.
Overall miasmatic conclusion: Child is born with fundamental load of sycosis++ and tubercular ++miasms, but does not carry any dominant load.
Final remedy with differentiation
[Table 4] shows repertorial syndrome and remedial coverage. Anger with its characteristic expressions and aversion to company is the core, covered by the Natrum group more than Calc Carb and Phos. Strong physical general symptoms milk aggravation is covered only by Nat Carb[19] and Chamomilla.[20] The final choice was Nat Carb.
| Repertorial syndrome | |
|---|---|
| 1. Irritability on contradiction | Craving: |
| 2. Clenching teeth anger during | 1. Cold drinks+++ |
| 3. Aversion to company | 2. Ice cream+++ |
| 4. Aversion touched being | 3. Sweets+++ |
| 5. Reserved | 4. Pica++ |
| 6. GIT complaints < Milk after | 5. Oranges++ |
| 7. Thumb sucking | 6. Cakes++ |
| 8. No bowel/ bladder control |
Remedies: Calc. Carb 22/13, Phos 21/13, Nat. Mur 17/8, Ignatia 16/7
The core of this case is anger: She gets angry at the slightest contradiction and expresses herself by clenching her teeth. Along with anger child is reserved, has aversion for company and does liked to be touched. All these expressions indicate the Natrum personality, despite Calc. Carb being ahead in the numerical totality. Therefore, a remedy from the Natrum group that also covers the keynote and qualified symptom (milk aggravation) is required. Natrum Carb is the only remedy covering that symptom. Considering the characteristic qualified mental symptoms and aggravating modality, Nat Carb is the simillimum.
Remedy selected: Natrum Carb, a Syco-tubercular remedy.
Potency and repetition: Nat Carb 200 C 1 dose weekly to 3 doses weekly.
Follow-up result: Her speech improved within 4–8 weeks. Her social interactions improved within 8–10 months to the extent that she started participating in elocution competitions and won in her later part of treatment. She did not require anti-miasmatic remedy.
DISCUSSION
All cases were studied based on the following parameters:
Onset of disease: Cases with early onset by the 1st year of life (1 and 2) have a more severe presentation. Cases with onset after 3 years (3 and 4) have a more intense dispositional expression with mild disease expressions.
Pace of disease: Pace of disease is rapid in Cases 1 and 2 and gradual in Cases 3 and 4.
Clinical presentation: All cases have more intense common expressions of ASD. Younger patients had more severe presentations (Cases 1 and 2); older patients (Cases 3 and 4) showed more dispositional symptoms with common presentations.
Presence of comorbidity: Cases with severe presentations had structural disturbances in the brain (Cases 1 and 2), while Cases 3 and 4 had functional complaints (allergic complaints).
All cases had individualistic presentations with ASD that was also characteristics expressions. For example, Case 1: Intense incessant hurting self, which was his nature. Case 2: Regressive symptoms with spitting. Case 3: Desire for cleanliness, perfectionism and travelling along with screaming in public and weeping at loud noises. Case 4: Difficulty in communication and followed instructions mechanically that is, dispositional qualities were glaringly available.
Mental state of mother during pregnancy: Disturbed mental state before and during conception affected the severity of disability (Cases 2 and 3); in Cases 1 and 4, this factor was absent. Tubercular miasm in the mother has travelled more deeply to syphilitic miasm in Cases 1 and 2. In Cases 3 and 4, sycotic influences are greater. Presence of multiple infections in the mother before conception indicate Tubercular load; in Case 2, prolonged low mood with secondary infertility indicates sycotic load. Cases 1 and 2 had significant maternal illnesses during pregnancy and anticipatory anxiety at delivery; they showed early signs of ASD. Cases 3 and 4 did not show depressive anxiety; complaint onset severity of expressions was mild.
Medical history: Tubercular-syphilitic miasm in medical history led to greater severity in Case 1; in Case 2, only Tubercular miasm caused severe presentation of ASD.
Family history: Tubercular-syphilitic miasm as a fundamental miasm produced tubercular-syphilitic presentation of ASD in Case 1, while the remaining cases have more of a sycotic load.
All the cases teach us that the time of onset of expression of disease and the pace of progress plays a major role in deciding miasms (Cases 1 and 3). The fundamental and dominant history has a role in deciding the miasm (Case 2 and 3). Susceptible constitution along with the individual susceptibility decides the presentation of disability. Maternal mental health and mental state around the time of pregnancy and post-delivery play a significant role in the disease process (Case 2 and 3).
This study emphasises that miasmatic background of remedies has a major role in the effectiveness of treatment.
CONCLUSION
There is a strong role of fundamental load in the development of ASD in all the cases –heavy fundamental load produces more severe forms of ASD.
Children having a strong sycotic and syphilitic miasmatic load in terms of fundamental and dominant load are more prone to intense expressions of ASD; disease expressions come up and progress rapidly.
Early age of onset in cases of tubercular and syphilitic miasm demonstrated slow pace of recovery.
Presence of dominant sycotic load showed normal development till they attained some milestones during developmental age and deviation started subsequently with a gradual pace.
Homoeopathic medicines with miasmatic qualities help resolve miasmatic blocks.
Constitutional treatment that is, ‘individualised and holistic management where comprehensive disease diagnosis, disease characteristics, analysis of susceptibility and sensitivity and miasmatic load (fundamental/dominant) is considered when planning the treatment[1,3,5] yields better response.
Acknowledgement
Dr. Kumar M. Dhawale, Former Principal, HOD, Department of Psychiatry; MLDMHI for guidance and medical officers and residents from the Department of Psychiatry for unconditional help and parents who showed faith on homoeopathy.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Pervasive developmental disorder In: Sadock B, ed. Kaplan and Sadock’s Comprehensive Textbook of Psychiatry (9th ed). Philadelphia, PA: Lippinkott Williams and Wilkins; 2009. p. :3540-50.
- [Google Scholar]
- Prevalence of autism spectrum disorder in Indian children: A systematic review and meta-analysis. Neurol India. 2019;67:100-4.
- [CrossRef] [PubMed] [Google Scholar]
- Environmental factors influencing the risk of autism. J Res Med Sci. 2017;22:27.
- [CrossRef] [PubMed] [Google Scholar]
- Principle and Practice of Homoeopathy. (7th ed). New Delhi: B. Jain Publisher Private Ltd.; 2018.
- [CrossRef] [Google Scholar]
- Standard Treatment Guidelines in Homoeopathy-Autism Spectrum Disorder New Delhi: Central Council For Research in Homoeopathy; 2019. p. :13-25.
- [Google Scholar]
- Perceiving the mental state In: Symposium Volume. Area B-1. Mumbai: Dr. M.L. Dhawale Memorial Trust; 2014. p. :B2-8.
- [Google Scholar]
- Theoretical part In: The Chronic Diseases. New Delhi: B. Jain Publisher; 2007. p. :21-49.
- [Google Scholar]
- Calc carb In: Lectures on Homoeopathic Materia Medica. New Delhi: B. Jain Publisher Private Ltd.; 2002. p. :311-29.
- [Google Scholar]
- Lycopodium. In: Lectures on Homoeopathic Materia Medica. New Delhi: B. Jain Publisher Private Ltd.; 2002. p. :703-13.
- [Google Scholar]
- Tarentula hispanica In: The Arcana of Materia Medica (3rd ed). Netherland: Emryss Publication; 2004. p. :1337-48.
- [Google Scholar]
- Tarentula hispanica In: Lectures on Homoeopathic Materia Medica. New Delhi: B. Jain Publisher Private Ltd.; 2002. p. :990-4.
- [Google Scholar]
- Tuberculinum In: Lectures on Homoeopathic Materia Medica. New Delhi: B. Jain Publisher Private Ltd.; 2002. p. :1001-7.
- [Google Scholar]
- Carcinosin In: Soul of Remedies. Mumbai: Homoeopathic Medical Publishers; 2017. p. :55-9.
- [Google Scholar]
- Stramonium In: Lectures on Homoeopathic Materia Medica. New Delhi: B. Jain Publisher Private Ltd.; 2002. p. :948-51.
- [Google Scholar]
- Artificial Drug Disease: Perceiving: Calcarea Disease Symposium (3rd ed). Mumbai: Dr. M.L. Dhawale Memorial Trust; 2014. p. :F27-41.
- [Google Scholar]
- Calcarea phos In: Lectures on Homoeopathic Materia Medica. New Delhi: B. Jain Publisher Private Ltd.; 2002. p. :334-7.
- [Google Scholar]
- Natrum carbonicum In: Lectures on Homoeopathic Materia Medica. New Delhi: B. Jain Publisher Private Ltd.; 2002. p. :762-6.
- [Google Scholar]
- Chamomilla In: Lectures on Homoeopathic Materia Medica. New Delhi: B. Jain Publisher Private Ltd.; 2002. p. :414-24.
- [Google Scholar]




