
Translate this page into:
Management of ovarian cyst through sepia given in LM potency – Case series
*Corresponding author: Dr. Padmalaya Rath, Scientist - 3, Dr. D. P. Rastogi Central Research Institute for Homoeopathy, Noida, Uttar Pradesh, India. drpadmalaya@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Rath P, Saraswat K. Management of ovarian cyst through sepia given in LM potency – Two case reports. J Intgr Stand Homoeopathy 2023;6:53-60.
Abstract
Ovarian cysts are benign growths arising from the ovary, usually occurring in women of reproductive age. Ovarian cysts are fairly common in clinical practice and may be diagnosed symptomatically or incidentally through investigations like ultrasound sonography. This article reports two cases of women with ovarian cysts who were treated successfully with individualised homoeopathic medicines. The medicines were prescribed in fifty millesimal (LM) potency, based on homoeopathic principles of individualisation. The cases were further observed for 12 months without recurrence of symptoms. Both patients were assessed at baseline and end of treatment for pain using the visual analogue scale score and ultrasound reports. During treatment, both patients followed up every 20 days. After treatment ended, they were further observed for 12 months for symptom recurrence. In the second case, the MONARCH score was +7/13, indicating a positive causal attribution of homoeopathy in resolution of the pathological ovarian mass. Favourable results were observed through homoeopathic constitutional approach to ovarian cysts. Symptomatic relief and objective changes were seen, along with no recurrence of the symptoms and cysts. Homoeopathic Individualized medicines prescribed in fifty millesimal potency can serve beneficially in the management of surgical cases like ovarian cysts.
Keywords
Homoeopathy
Individualised homoeopathic treatment
LM potency
Ovarian cyst
Sepia

INTRODUCTION
Ovarian cysts are predominantly benign growths arising from the ovaries. These lesions may be diagnosed symptomatically or incidentally. The common ovarian lesions include physiological cysts, endometrium, benign cystic teratoma and cystadenoma. Malignant lesions are comparatively rare.[1]
Ovarian cysts are more common in women of reproductive age. The incidence is slightly higher in girls at the age of menarche. While most ovarian cysts are benign, the risk of malignancy is higher in post-menopausal women.[1,2]
Some ovarian cysts can be functional, such as follicular cysts. These occur when the follicle does not open and release the egg cell; the follicle occasionally fills up with fluid and a cyst develops. A corpus luteum cyst occurs when a corpus luteum fills with blood. Theca lutein cysts may develop in women who undergo infertility treatment with hormones. Chocolate cysts (endometriomas) are filled with dark, thick blood and develop as a result of endometriosis.
Dermoid cysts (which are not functional cysts) contain matter such as skin cells and sebaceous glands; these are less common and may develop from non-cancerous tumours.[2]
The most common complications are rupture, bleeding and twisting of the cyst around its blood supply, known as torsion.
According to an extensive French study, the number of hospital stays for benign ovarian tumours or ovarian cysts was 45,000 in 1998 and 1999. Nearly 7000 women were hospitalised for follicular or yellow body cysts, that is, 15%, with an incidence of 29/100,000 women over the age of 15 years. Serous and mucinous cysts account for 20–30% of the operated cysts and dermoid cysts for 10–20%.[3]
Homoeopathy is a system of medicine that focuses on individualisation to select the required remedy. Surgical cases like ovarian cysts have shown promising results with homoeopathy.[4-10]
Literature states that the 50-millesimal potency has been shown to be the most effective in dealing with similar conditions.[11-13]
According to a research published in 2022, titled ‘Noninvasive Resolution of Pathological Ovarian Masses with Homoeopathic Treatment – A Case Series’, complete resolution of the ovarian cysts occurred in all cases, evidenced by ultrasonography (USG). The patients improved within 4–15 months of treatment using individualised homoeopathic medicines.[11] In another research published in 2011, titled ‘Evidence-based clinical study on the effect of homoeopathic medicines in cases of ovarian cysts’, a total of 73 patients suffering from ovarian cysts were enrolled, (48 completed the study) according to protocol. Medicines were selected on the basis of individualisation and changes in the size of ovarian cysts were assessed at the end of 1 year. After comparing pre- and post-treatment USG reports, the difference in mean values of the maximum dimension of the ovarian cyst was found to be statistically significant.[5]
CASE SERIES
This article comprises of case reports (almost decade apart) of two females suffering from ovarian cyst, cured with Homoeopathic medicine Sepia based upon individualization of symptoms and using LM potency.[13]
CASE 1
Presenting complaints
A 19-year-old unmarried woman reported on 20 April 2010 with complaints of delayed menses and pain in the left iliac region of the abdomen. She also reported occasional episodes of experiencing internal and external heat/flushes in the genitals. She had menorrhagia and dysmenorrhoea. She also reported acne with intense itching aggravated before menses. She also reported occasional whitish discharge per vagina. Her USG report was suggestive of a left-sided ovarian cyst [Figure 1].
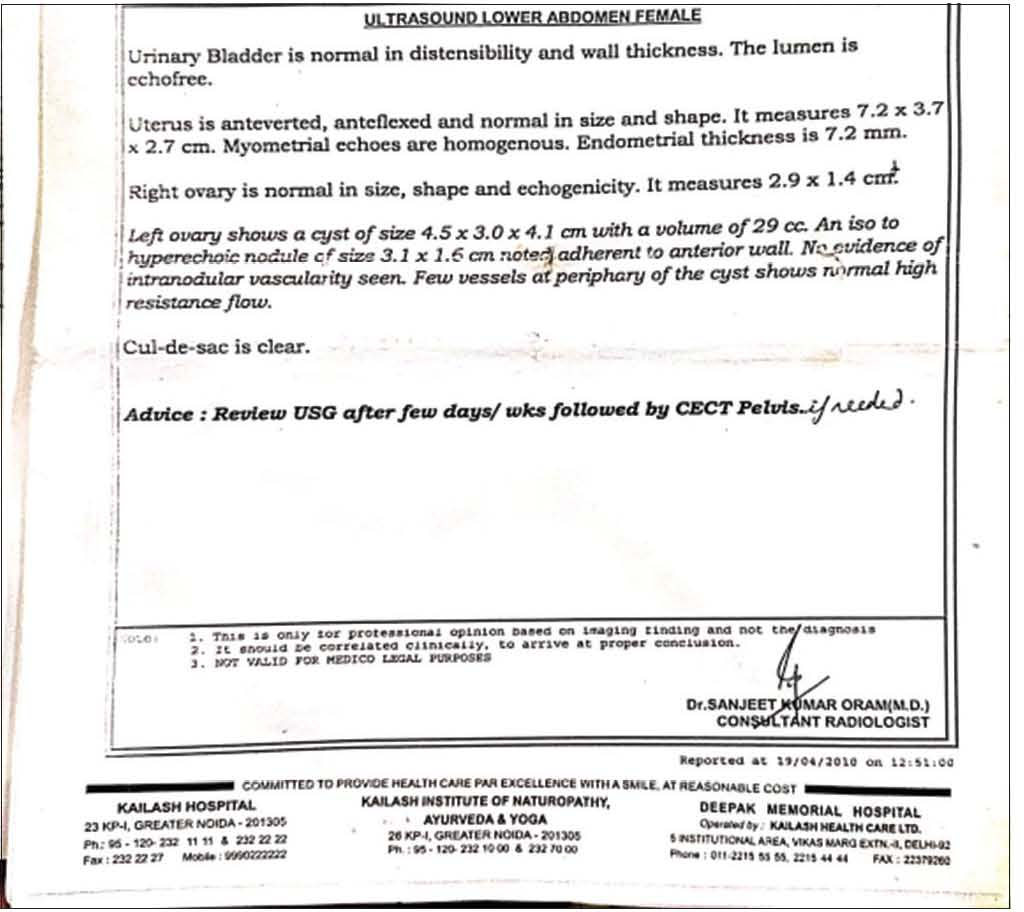
- USG report- Pre treatment.
Physical generals
The patient’s thermal reaction was towards chilly. She was very fond of sweets. Perspiration was slightly offensive and profuse.
Mental generals
She was very ambitious and a workaholic. She was very concerned about her future and developed anxiety and headaches if too occupied with thoughts or work. She always desires to be occupied. She said she communicates well with others, but when she is emotionally affected, she is unable to do so. Irritability at trifles, especially during menses. Audacity was a marked symptom noted while case taking.
Totality of symptoms
Totality was built on the basis of Kent’s approach, considering mental symptoms at the top followed by Generals (Physical and mental) and Particulars. The repertory used was synthesis using RADAR software developed in Archibel Belgium.
Ambitious
Audacity
Desire to remain occupies
Cannot tolerate advice by others
Cannot tolerate contradiction
Anger easily and violent
Irritable on trifles
Headache with anxiety
Confused when she wakes up in the morning
Chilly patient
Sweets desire
Acne on face
Acne aggravated before menses
Ovarian cyst
Profuse menses
Painful menses
Baseline prescription
Based on repertorisation [Figure 2] and Materia Medica references, Sepia 0/1/OD was prescribed on the first visit on 20 April 2010 for 20 days. Materia Medica confirmed the symptoms and totality. The following Materia Medica books were studied: Hering Guiding Symptoms of our Materia Medica, The Clinical Materia Medica by JH Clarke and Lectures on Homoeopathic Materia Medica by Kent.[14-18] Table 1 outlines the complete follow up of the case. USG advised after the treatment reported normal findings [Figure 3]. Her VAS score at initial visit was 9 [Figure 4].

- Repertorial Sheet case 1.
| Date | Symptoms | Medicine | Outcome |
|---|---|---|---|
| 10 May 2010 | Pain in the left iliac region of the abdomen – better Internal and external heat in genitals – slightly better Acne with itching – same |
Sepia 0/2/OD/20 days | There was initial relief of symptoms, followed by status quo |
| 30 May 2010 | Menses (LMP – 27 May 2010) Dysmenorrhoea-same as before Pain in left iliac region of abdomen-better Internal and external heat in genitals-slightly better Acne with itching – slightly better |
Sepia 0/3/OD/20 days | There was marked relief of symptoms, but dysmenorrhea present as before (LMP- May 27, 2010) |
| 20 June 2010 | Pain in the left iliac region of abdomen – better Internal and external heat in genitals – slightly better Acne with itching – slightly better |
Sepia 0/4/OD/20 days | There was marked relief of symptoms, but they some repeated in between (abdominal pain and acne) |
| 10 July 2010 | Menses LMP – 26 June 2010, Dysmenorrhoea present Pain in the left iliac region of abdomen – episodes of increased pain in between Internal and external heat in genitals – still persistent Acne with itching – slightly better |
Sepia 0/5/OD/20 days | LMP – 26 June 2010, Flow was normal. Dysmenorrhoea was still present with marked relief in other symptoms. |
| 1 August 2010 | Menses LMP – 27 July 2010, dysmenorrhea better Pain in the left iliac region of abdomen – better Internal and external heat in genitals – still persist Acne with itching – better |
Sepia 0/6/OD/20 days | There was marked relief of symptoms, with occasional reoccurrence of a few of the symptoms |
| 21 August 2010 | Pain in the left iliac region of abdomen-better Internal and external heat in genitals – better Acne with itching – few new acne noted |
Sepia 0/7/OD/20 days | Relief of symptoms |
| 11 September 2010 | LMP – 28 August 2010. No dysmenorrhea Pain in the left iliac region of abdomen – better Internal and external heat in genitals – better Acne with itching – better |
Sepia 0/7/OD/20 days | Relief of symptoms. Same potency was repeated |
| 31 September 2010 | Pain in the left iliac region of abdomen – better Internal and external heat in genitals – better Acne with itching – some new pimples over forehead noted. |
Sepia 0/8/OD/20 days | General condition of patient was much better. Itching in acne was reduced, but she noted some new pimples in between. Potency raised |
| 21 October 2010 | Pain in the left iliac region of abdomen – better Internal and external heat in genitals-better Acne with itching-better |
Sepia 0/8/OD/20 days | Relief of symptoms. Same potency was repeated |
| 1 November 2010 | Pain in the left iliac region of abdomen – better Internal and external heat in genitals – better Acne with itching – better |
Sac lac 0/9/OD/20 days | Relief of symptoms. USG advised |
| 30 December 2010 | Pain in the left iliac region of abdomen – better Internal and external heat in genitals – better Acne with itching – better |
Sac lac 0/9/OD/20 days | USG report was normal [Figure 3]. There was no need of further intervention. Still for satisfaction of patient, placebo was given for next 20 days VAS score (for pain)-1 |
VAS: Visual analogue scale, USG: Ultrasonography

- USG report- Post treatment.
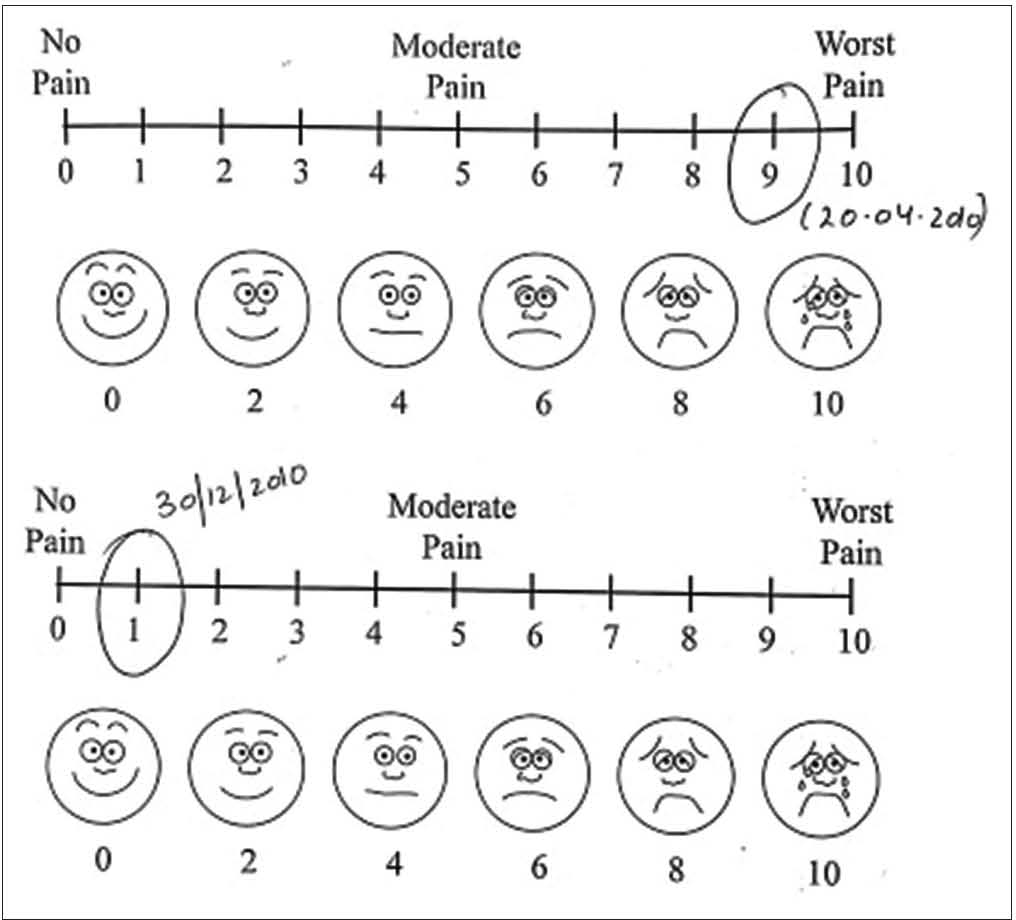
- Pre and post VAS score of patient 1.
CASE 2
Presenting complaints
A 44-year-old patient presented with complaints of pain in the lower abdomen for 2 weeks, profuse menses for 2–3 months. Burning micturition on and off since 3 weeks. Discharge per vagina for 6 months. Pain in lower back for 2 months. Aggravation – especially during menses. Headache on and off at the time of menstruation. Chronic constipation for 2 years. She brought her USG reports [Table 2, Figures 5 and 6].
| 14 December 2020 | Fatty Liver Grade I, Left adnexa shows well defined cystic lesion showing fine fibrous strands in cystic mass s/o haemorrhagic/complex cyst 4.28×4.26×4.92 cm Concretions in both kidneys |
|---|---|
| 15 December 2020 | Bilateral complex ovarian cyst |
| 13 June 2021 | Normal ultrasonography findings |

- Repertorial sheet case 2.
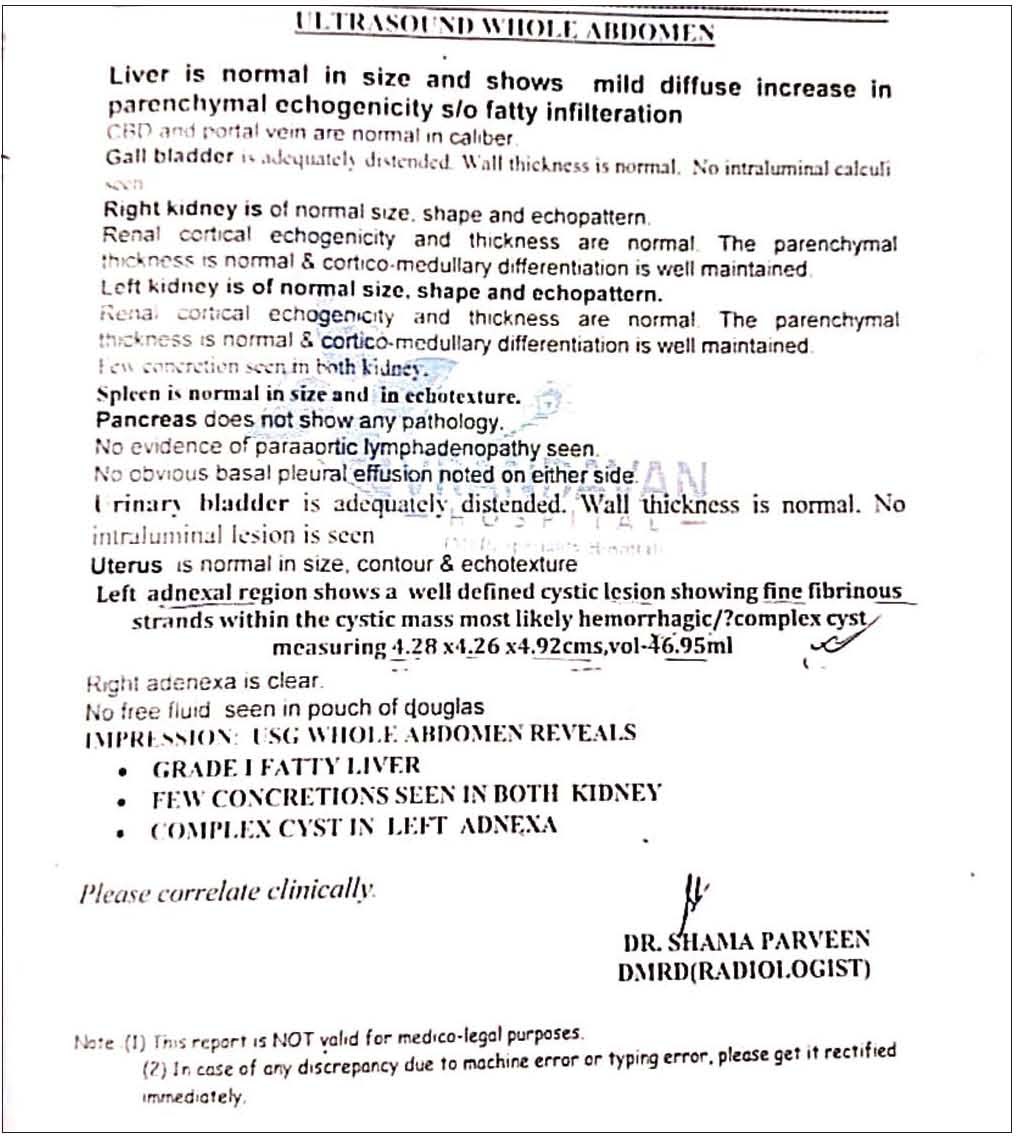
- USG report- Pre treatment.
Physical generals
The thermal reaction was towards chilly. Appetite was good. Thirst adequate. Desires salty things. Perspiration was generalised. Stools were unsatisfactory with constipation.
Mental generals
The patient was frank and forthcoming with her issues. She was quite active and desires to remain occupied always, which gives her a sense of mental satisfaction. She did not like anyone giving her any sort of advice. She cannot bear contradiction. On communicating with her, she appeared to be ambitious (for herself as well as her children). Her anger is violent; although she is not destructive, she gets impulses to break things in anger.
Investigations
Investigations are mentioned in Table 2. USG reports before treatment [Figures 6 and 7] and after treatment [Figure 8].
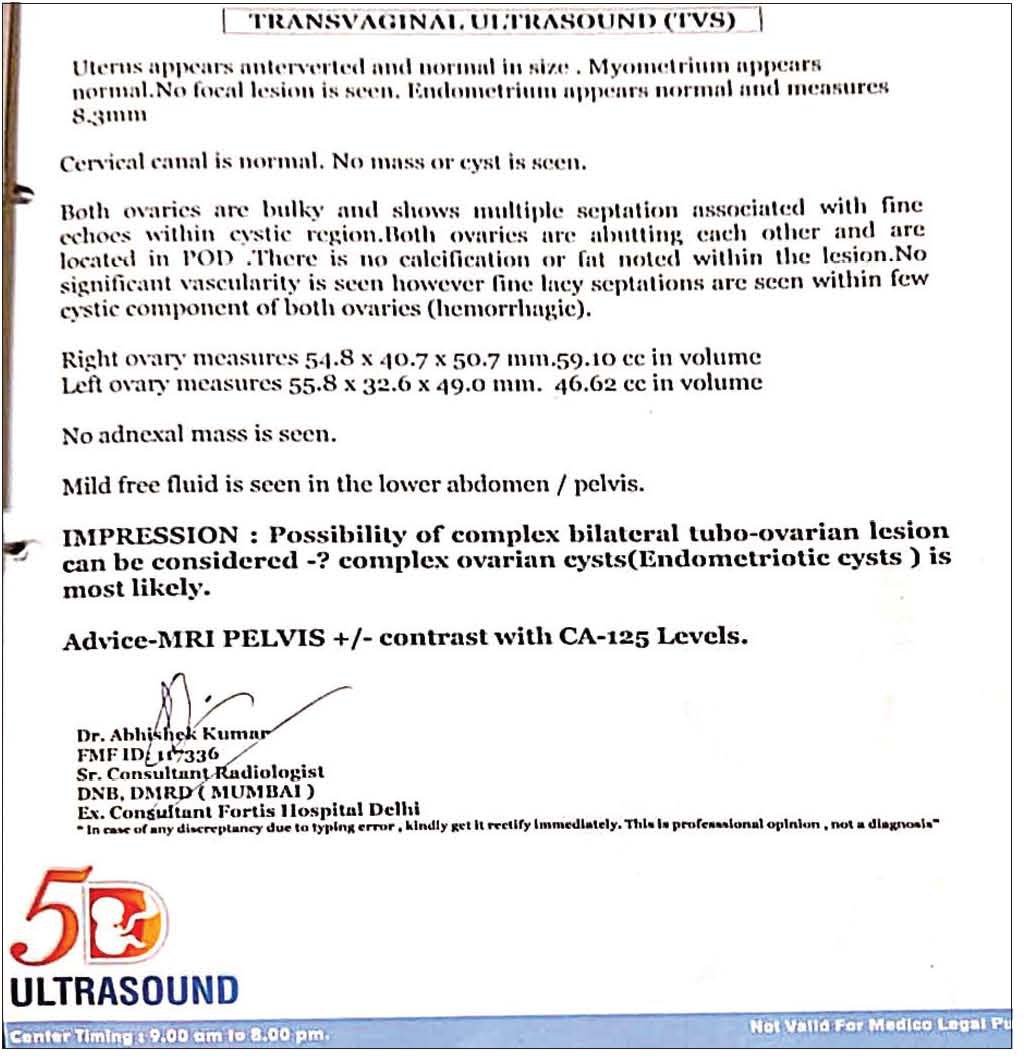
- USG report- Pre treatment.
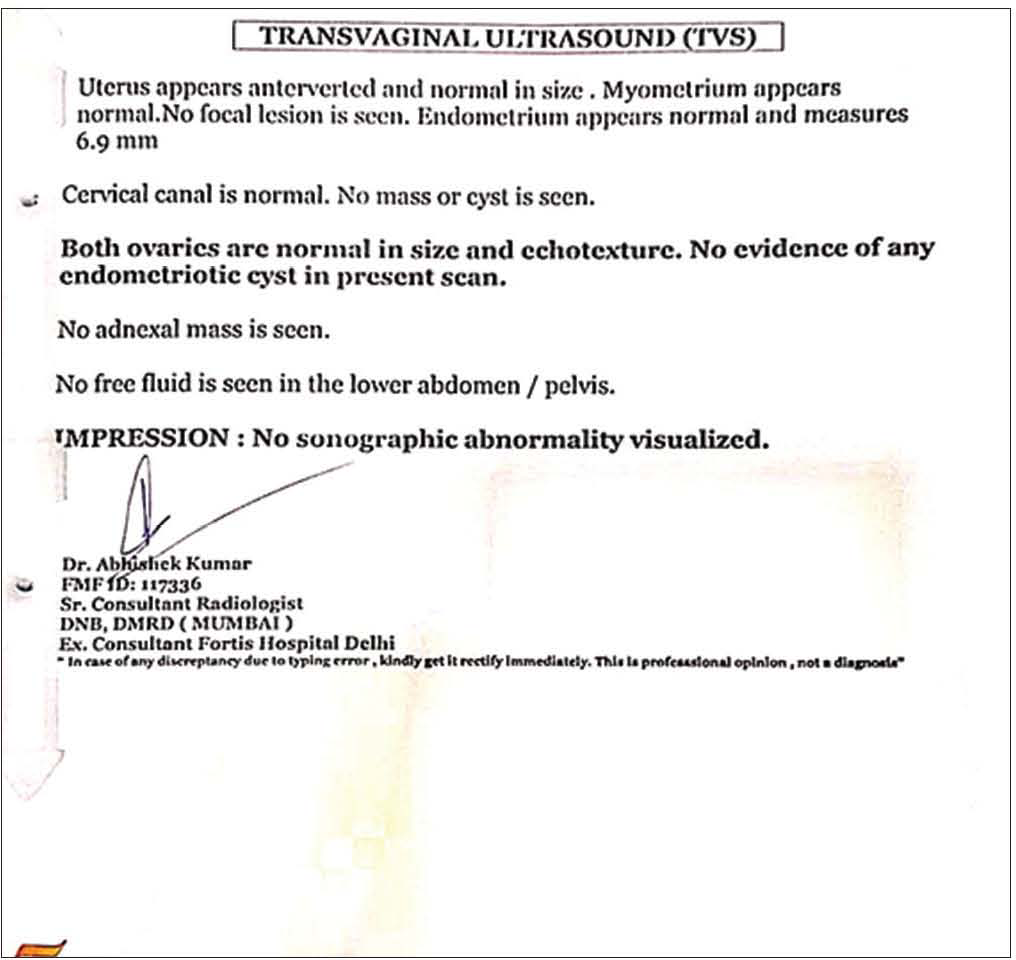
- USG report- Post treatment.
Totality of symptoms
Totality was built on the basis of Kent’s approach, considering mental symptoms at the top followed by ‘Generals’ (Physical and Mentals) and ‘Particulars’ thereafter. The repertory used was synthesis using RADAR software developed in Archibel Belgium.
Audacity
Aversion to company
Desire to remain occupied
Cannot tolerate advice
Contradiction aggravation
Angered easily
Chilly patient
Desire for salt
Pain lower abdomen
Constipation
Burning urination
Profuse menses
Thick leucorrhoea
Ovarian cyst.
Baseline prescription
On repertorial analysis, sepia was found to be the similimum. Materia Medica[14,15] pointed towards the same.
Remedy and posology
Sepia 0/1 BD for 20 days was prescribed on 30 December 2020. Table 3 outlines complete follow up of the case.
| Date | Symptoms | Medicine | Justification |
|---|---|---|---|
| 20 January 2021 | Pain in lower abdomen – slightly better Burning micturition – slightly better Discharge per vagina – slightly better Pain in lower back – same Constipation – slightly better |
Sepia 0/2/OD/20 days | There was mild initial relief of symptoms, but status quo later |
| 25 February 2021 | Pain in lower abdomen – slightly better Burning micturition – better Discharge per vagina – better Pain in lower back – same Constipation – slightly better |
Sepia 0/3/OD/20 days | There was marked initial relief of symptoms, especially leucorrhoea and burning micturition but later on status quo |
| 23 March 2021 | Pain in lower abdomen – on and off Burning micturition – better Discharge per vagina – on and off Pain in lower back – on and off Constipation – better |
Sepia 0/4/OD/20 days | There was marked relief of symptoms, but they get repeated in between (leucorrhoea, abdominal pain, lower back pain) |
| 12 May 2021 | Pain in lower abdomen – better Burning micturition – relief Discharge per vagina – relief Pain in lower back – better Constipation – better |
Sepia 0/5/OD/20 days | All the complaints were much better, but few still present. Therefore, raised potency was given and patient was advised to get her USG done. |
| 16 June 2021 | Pain in lower abdomen – relief Burning micturition – relief Discharge per vagina – relief Pain in lower back – relief Constipation – better |
Sac lac 0/6/OD/20 days | USG report was normal [Figure 7]. There was no need for further intervention. Still for satisfaction of patient, placebo was given for next 20 days VAS Score (for pain) was 0 |
VAS: Visual analogue scale, USG: Ultrasonography
Follow-ups
Follow up of the given case is mentioned in detail in Table 3 along with justification of the prescription. MONARCH Score at the end of treatment was 7/13 [Table 4].
| Items | Yes | No | Not sure |
|---|---|---|---|
| 1. Was there an improvement in the main symptom or condition, for which the homoeopathic medicine was prescribed? |
+2 | ||
| 2. Did the clinical improvement occur within a plausible time frame relative to the drug intake? | +1 | ||
| 3. Was there an initial aggravation of symptom? (need to define in glossary | 0 | ||
| 4. Did the effect encompass more than the main symptom or condition that is, were other symptoms ultimately improved or changed? |
0 | ||
| 5. Did overall well being improve? | +1 | ||
| 6. (a). Direction of cure: Did some symptoms improve in the opposite order of the development of symptoms of the disease? |
0 | ||
| (b). Direction of cure: Did at least two of the following aspects apply to the order of improvement of symptoms: • From organs of more importance to those of less importance • From deeper to more superficial aspects of the individual • From the top downwards |
0 | ||
| 7. Did ‘old symptoms’ (defined as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? | 0 | ||
| 8. Are there alternate causes (other than the medicine) that – with a high probability – could have caused the improvement? (Consider known course of disease, other forms of treatment and other clinically relevant interventions) |
+1 | ||
| 9. Was the health improvement confirmed by any objective evidence? (e.g., laboratory test, clinical observation) | +2 | ||
| 10. Did repeat dosing, if conducted, create similar clinical improvement? | 0 |
VAS Score pre-post [Figure 9].
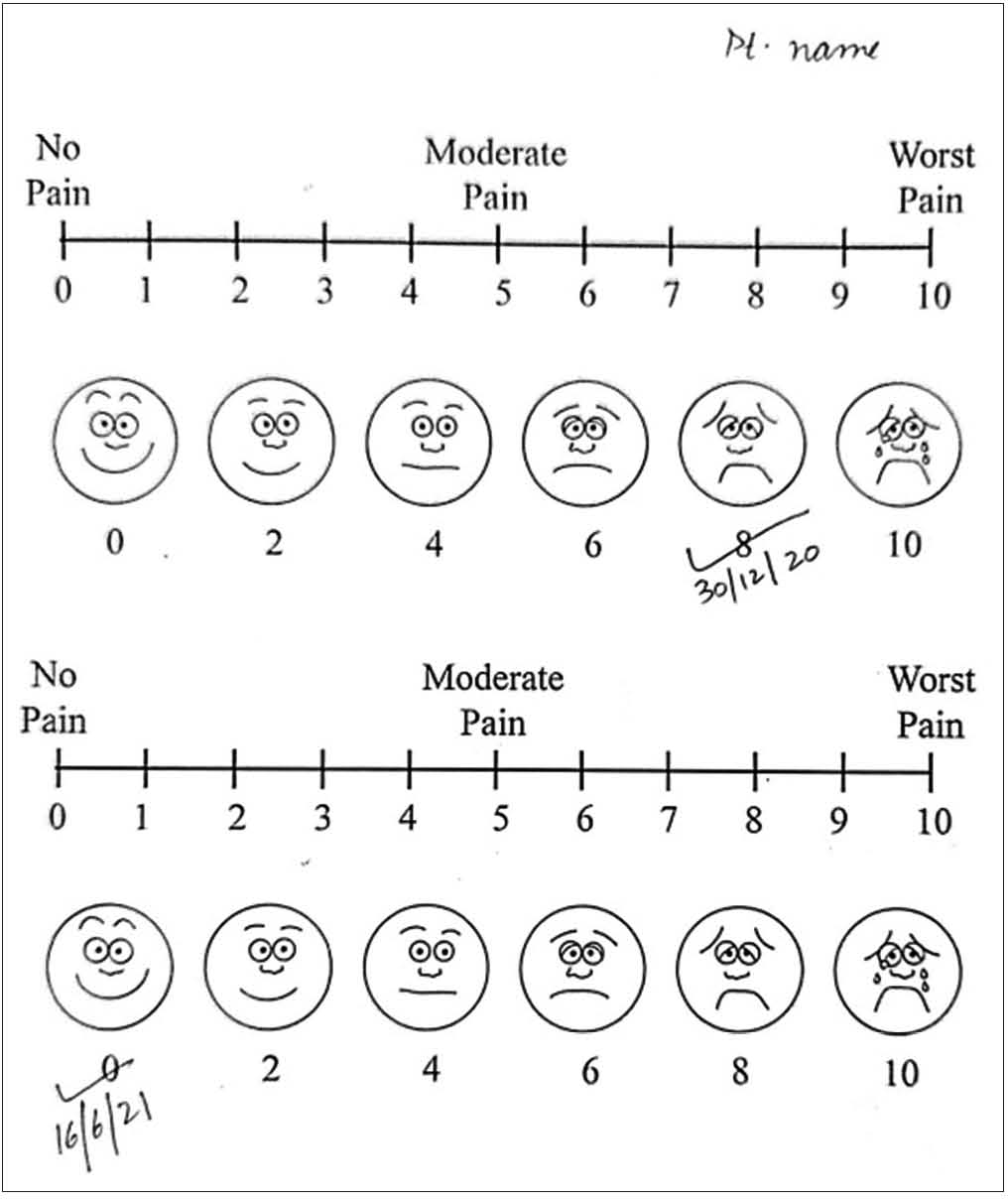
- Pre and post VAS score of patient 2.
DISCUSSION
These cases have shown encouraging results with homoeopathic treatment. It is important to note that patients with ovarian cysts need to be assessed on mental and physical aspects for better prescription. In both the cases, individualisation was done on the basis of mental symptoms and dispositional characteristics of the patients were considered during prescription.
The first case report supports the findings of previous studies[6,7,19] and a study by Gupta et al.[5] where after comparing pre- and post-treatment USG reports, the difference in mean values of maximum dimension of ovarian cyst was found to be statistically significant. The useful homoeopathic medicines in this study[5] were Natrum muriaticum, Pulsatilla, Sepia, Calcarea carb, Silicea, Arsenic alb and Phosphorus, which are almost similar to the constitutional medicines used in the previous studies. Sulphur and Carcinosin were the two medicines additionally prescribed in previous studies. A study conducted by Bukhsh et al. reported that large ovarian cysts in three patients were cured by the use of different potencies of the single remedy Thuja occidentalis; this study concluded that proper selection of the homoeopathic remedy considering the symptom totality can remove cysts from the ovary without any surgical intervention.[8] A study by Das et al. indicates that proper selection of the homoeopathic remedy considering the symptom totality and in consultation with repertory can remove cysts from the ovary without any surgical intervention.[9]
In the second case report, the modified Naranjo score of the patient after treatment was 7 [Table 4], which indicates there is a likelihood of causality between the result observed and the prescribed homoeopathic medicine in the case. This concurs with the study[4] where The MONARCH score was calculated as +7/13, +9/13, and +9/13 for the three cases, respectively, indicating a positive causal attribution of homoeopathy in the resolution of these pathological ovarian masses. This report also supports previous studies where the patients improved within 4–15 months of treatment using individualised homoeopathic medicines.[4,5] A case study by Nath et al. reports that the medicine was selected based on the totality of symptoms by referring to Repertorium Homoeopathicum Syntheticum and Materia Medica, yielding Lycopodium clavatum as the similimum. The patient’s general well-being improved; pre- and post-treatment USG reports proved the cure.[10]
CONCLUSION
Individualisation is defined as a process of differentiating one person from others by some peculiar or unique features and a remedy is given accordingly. This article represents case reports of two such cases cured with an individualised homoeopathic approach, where medicines were given in LM potency. Homoeopathy not only showed promising results by improvement in patients’ symptoms but evidence in the form of USG reports justifies the cure. It can be concluded that homoeopathic therapy may reduce the burden of surgeries for ovarian cysts and may be considered as a viable treatment before considering surgery.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Shaw’s Textbook of operative gynaecology United States of America: Churchill Livingstone; 1977.
- [Google Scholar]
- Ovarian Cyst In: StatPearls. Treasure Island: StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560541 [Last assessed on 2022 Oct 05]
- [Google Scholar]
- Epidemiology of apparently benign ovarian cysts. J Gynecol Obstet Biol Reprod (Paris). 2001;30:S8-11.
- [Google Scholar]
- Non-invasive resolution of pathological ovarian masses with homoeopathic treatment-a case series. Homoeopathy. 2022;111:194-201.
- [CrossRef] [PubMed] [Google Scholar]
- Evidence based clinical study on the effect of homoeopathic medicines in cases of ovarian cysts. IJRH. 2011;5:36-42.
- [CrossRef] [Google Scholar]
- A clinical study on cases of pelvic tumours in response to homoeopathic treatment assessed by ultrasonography. Asian Homoeopathic J. 1995;5:15-23.
- [Google Scholar]
- Ultrasonographic follow-up of ovarian cyst cases in response to homoeopathic treatment: A clinical study. Ayush. 2006;2:1-15.
- [Google Scholar]
- Removal of large sized ovarian cysts in three patients by administration of a single remedy, Thuja occidentalis: Hormonal assay and ultrasonographic images. J Integrative Med Ther. 2016;3:9.
- [CrossRef] [Google Scholar]
- Removal of large sized ovarian cysts by potentized homoeopathic remedies: A myth or a dependable alternative option. Int J Complement Alt Med. 2016;3:088.
- [CrossRef] [Google Scholar]
- Homoeopathic management of ovarian cyst-a case report. Int J Res Ayush Allied Syst. 2019;6:2393-9.
- [CrossRef] [Google Scholar]
- My Experiments with 50 Millesimal Scale of Potency In: Reprint (5 th ed). Kottayam, Kerala: Hahnemann Homoeopathic Pharmacy publisher; 1986. p. :73.
- [Google Scholar]
- Hahnemann's experiments with 50 millesimal potencies: A further review of his casebooks. Homoeopathy. 2006;95:171-81.
- [CrossRef] [PubMed] [Google Scholar]
- Lectures on Homoeopathic Materia Medica New Delhi: B. Jain Publishers Pvt Ltd.; 2010.
- [Google Scholar]
- Guiding Symptoms of our Materia Medica New Delhi: B. Jain Publishers Pvt Ltd.; 2014.
- [Google Scholar]
- New Manual of Homoeopathic Materia Medica New Delhi: B. Jain Publishers Pvt Ltd.; 2014.
- [Google Scholar]
- Homoeopathic treatment of ovarian cysts-a series of 40 cases. Br Homoeopathic J. 1991;80:143-8.
- [CrossRef] [Google Scholar]




