
Translate this page into:
A holistic and individualised homoeopathic approach to adenomyosis – A case report
*Corresponding author: Dr. Sanjib Sahoo, Department of Materia Medica, Maa Kalawati Homoeopathic Medical College and Hospital, Ranchi, Jharkhand, India. pmsanjibsahoo970@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sahoo S, Mukherjee S, Roy B, Saha D, Mahato AP. A holistic and individualised homoeopathic approach to adenomyosis – A case report. J Intgr Stand Homoeopathy. 2024;7:166-72. doi: 10.25259/JISH_68_2023
Abstract
Adenomyosis is characterised by the presence of endometrial tissue within the uterine myometrium. Clinical symptoms include menorrhagia, dysmenorrhoea, dyspareunia, and infertility, all of which negatively affect the patient’s quality of life. Despite drastic advancements in modern medicine, the treatment and cure of adenomyosis without surgical intervention is still challenging. Homoeopathy, an alternative system of medicine, can successfully treat adenomyosis with potentised remedies, avoiding surgery. A 27-year-old multiparous woman, presented with dysmenorrhoea, menorrhagia, and white discharge per vagina for a prolonged period. The homoeopathic medicine Medorrhinum, prescribed based on strict individualisation, helped cure the patient. This case showed a favourable prognosis to a difficult gynaecological condition like adenomyosis with individualised homoeopathic treatment.
Keywords
Adenomyosis
Individualisation
Medorrhinum
Homoeopathy

INTRODUCTION
Adenomyosis is a benign gynaecological disorder defined as the presence of ectopic endometrial glands and stroma within the uterine myometrium. The histopathologic abnormality was first named cystosarcoma adenoids uterinum.[1] However, its epidemiology has drastically changed. Adenomyosis has long been thought of as a characteristic condition in multiparous women over 40 years old with pain and excessive menstrual bleeding. However, using imaging methods such as transvaginal ultrasound and magnetic resonance, adenomyosis has increasingly been discovered in young women who have pain, abnormal uterine bleeding, infertility, or no symptoms at all.[2,3] Although the pathogenic mechanisms behind adenomyosis still need to be fully understood, an increasing number of studies over the past 10 years have demonstrated that sex steroid hormone receptors, inflammatory molecules, extracellular matrix enzymes, growth factors, and neuroangiogenic factors play a significant role.[4,5] The most widely accepted explanation states that adenomyosis is caused by the invagination of basalis endometrium into the myometrium through a damaged or interrupted junctional zone, which is a highly specialised hormone-responsive structure found in the inner third of the myometrium[4] or is created entirely from the metaplasia of residual embryonic Müllerian cells.[4]Adenomyosis was formerly diagnosed primarily through histology examination.[6] As a result, its incidence or prevalence has not been precisely determined. Therefore, estimates of adenomyosis prevalence range greatly from 5% to 70%, with the typical frequency of adenomyosis at hysterectomy between 20% and 30%.[7,8] Adenomyosis remains an underdiagnosed condition due to a lack of pathognomonic symptoms.[9] Up to 30% of patients are asymptomatic; menorrhagia, dysmenorrhea, chronic pelvic discomfort, dyspareunia, and subfertility are some of the presenting symptoms.[10] Moreover, as endometriosis and fibroids frequently coexist and share similar clinical characteristics, diagnosing these conditions can be challenging.[9] With the introduction and development of ultrasound and magnetic resonance imaging, various criteria have been used to determine the differential diagnosis, assess the depth of myometrial invasion, and track treatment response.[11] Despite recent advancements in modern medicine in the treatment of adenomyosis, it still poses a significant challenge for clinicians. Gonadotropin-releasing hormone analogues, progestin, combined oral contraceptives, and non-steroidal anti-inflammatory drugs are conventionally used to treat adenomyosis. If conservative treatment fails, uterine artery embolisation or hysterectomy is performed; however, neither procedure ensures complete recovery.[12,13]
As there are potential adverse effects of allopathic treatment, including menopausal symptoms, irregular bleeding, amenorrhoea, and thromboembolic phenomena, an alternative approach is required. Homoeopathy, as a holistic system of medicine, aims at eradicating the disease to its whole extent by restoring order to the dynamically deranged vital principle.[14] It considers the psycho-physical aspect of each disease to individualise treatment for each patient. Thus, homoeopathy treats the patient and not the disease condition. Homoeopathy is based on the principle of minimum dose, so chances of adverse outcomes are minimal. As rightly written by Skinner, ‘Constitutional treatment alone was and is all that is necessary for successful treatment of all vaginal, uterine and ovarian diseases’.[15] In the present case, the patient was treated gently following strict individualisation, which resulted in not only symptomatic relief but also the complete resolution of the condition at the organ level.
CASE REPORT
Patient information
A 27-year-old woman reported to outpatient department (OPD) of National Institute of Homoeopathy, Kolkata with the complaints of severe dysmenorrhoea and menorrhagia since 2 years. The pain was located in the lower abdomen and extended toward the back and upper part of the thigh. The pain which lasted throughout the menstrual period starting from day 1 at times, became so severe that it made the patient unconscious. The pain was typically aggravated by motion (+) and warm application (+) and was relieved by hard pressure (++) and stretching the legs against a support (+++). The patient had a sickly pale countenance as she had heavy and protracted menstrual bleeding for nearly 2 years. She mentioned requiring 20–35 sanitary pads per menstrual period. The menstrual bleeding contained large clots.
Along with these distressing complaints, the patient had white discharge per vagina throughout the month for 1 year. The character of discharge was irritating, offensive, and at times bloody, like the washing of meat. The patient had not found relief with ayurvedic and allopathic medications as well as home remedies.
Medical history
During childhood, the patient had frequent asthmatic attacks. She was treated with allopathic medicines, which resolved the complaints. She developed pelvic inflammatory disease at the age of 18 years, 4 months after her wedding. She had delivered four babies within 8 years; all were full-term normal vaginal deliveries. All complaints started after her last delivery in the nearby Rural Hospital.
Family history
The patient’s mother had arthritis. Her father had chronic bronchial asthma.
Physical generals
Despite having a poor appetite, the patient could not tolerate hunger as it caused headaches and dizziness. Her thirst was excessive, and she had to wake up to drink water frequently at night as her throat became very dry (+++). She craved spicy food (+), sweets (++), and cold drinks; she had an aversion to milk and dairy products. Her bowel movements were regular. She had developed a urinary tract infection a few months prior, and while allopathic treatment cured the condition, she reported occasional burning micturition (+). She had scanty perspiration, mostly on the upper part of the body. Her sleep was disturbed; she often experienced insomnia for days together without any apparent reason (++). Thermally, the patient was hot with a burning sensation in the palms and soles, which were aggravated by covering up (+++). Her menstrual cycles were regular but heavy and painful. The menstrual blood was bright red with large dark clots.
Mental generals
Anxiety regarding her family’s economic status was a constant problem. She was forgetful regarding recent events (+++), while her remote memories were sound enough. She appeared to be greatly distressed by her complaints.
Clinical examination
Her blood pressure was 110/72 mmHg, and her pulse was 84 beats/min. A bimanual pelvic examination (BPE) was performed in the gynaecology OPD of the hospital after obtaining proper verbally informed consent. BPE revealed an enlarged uterus and diffuse tenderness at the hypogastrium. Findings related to the cervix and vagina were unremarkable.
Diagnosis
The patient presented with progressive dysmenorrhoea and menorrhagia for a prolonged duration, which had not resolved following standard treatment. She had a history of repeated childbirth without a healthy gap between pregnancies. BPE revealed a tender and enlarged uterus. All these facts suggested a diagnosis of adenomyosis. An ultrasound dated 24 February 2021 revealed early adenomyotic changes in the uterus, chronic cervicitis, and pelvic inflammatory disease of the right adnexa [Figure 1].
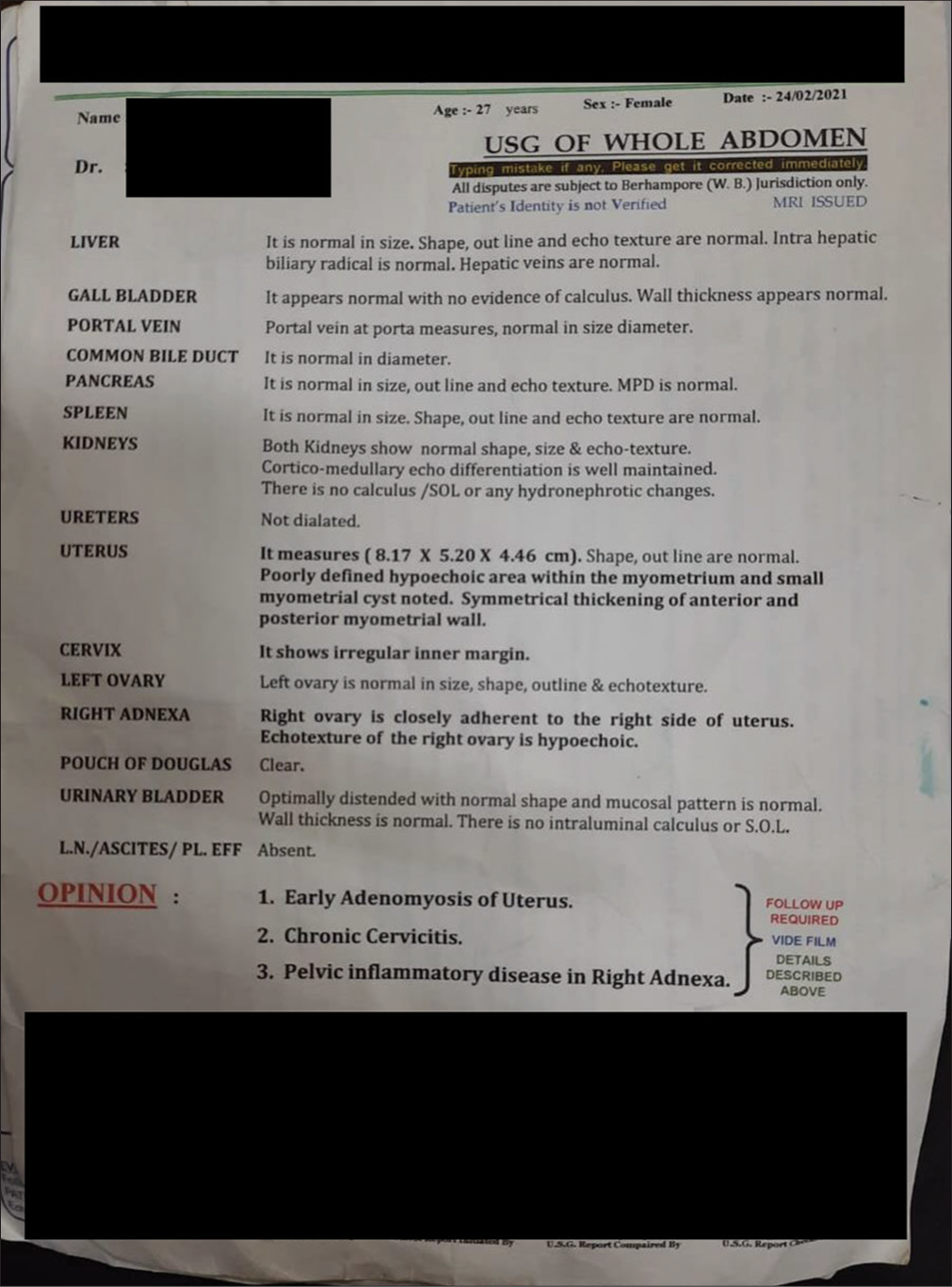
- Before treatment
The case was diagnosed as adenomyosis. N80.03 is the International Classification of Diseases, Tenth Revision, and Clinical Modification code for Adenomyosis.
Homoeopathic approach
Analysis of the case was performed following meticulous case-taking. Symptoms were evaluated following Kent’s method of evaluation which considers mental generals of the highest importance followed by characteristic physical generals and particulars. The case contained strong mental and physical generals and peculiar modalities. Therefore, the totality of symptoms, as well as the first prescription, was based on the characteristic generals and particular manifestations of the case, which individualised the patient.
Totality of symptoms
Great forgetfulness for recent memories (+++)
Extremely hot patient (+++)
Poor appetite, she could not tolerate hunger as it causes headache and dizziness
Excessive thirst aggravated at night (+++)
Craving for spicy food and sweets (++)
Insomnia without any apparent psychological cause (++)
Dysmenorrhoea aggravated by warmth (+) and motion (+)
Dysmenorrhoea relieved by stretching legs against a strong support and by hard pressure (+++)
Burning sensation over palms and soles; any covering aggravates it (+++)
Family history of arthritic disorders and bronchial asthma, which primarily belongs to the miasm Sycosis.
Therapeutic intervention
First prescription (28 March 2021)
Medorrhinum 200; 4 no. 10 globules to be dissolved in 10 mL distilled water. The entire preparation is to be taken in the morning on an empty stomach for 1 day.
Basis of first prescription
The patient’s forgetfulness, burning sensation of palms and soles with hot thermal reaction, desire for sweet, excessive thirst with dry throat at night compelling patient to drink water at night, dysmenorrhoea ameliorated particularly by stretching the legs against a strong support and strong sycotic family background clearly indicated Medorrhinum.[16] The 200th potency was selected based on the patient’s susceptibility and nature of the disease and medicine.
Results
At baseline, the patient was prescribed a single dose of Medorrhinum 200 on the basis of totality of symptoms. Some of the symptoms showed initial transient aggravation. The improvement of the case was steady and continuous following the first prescription. The medicine was repeated at different time points as suggested by the existing symptom complex. No other acute or intercurrent medicine was prescribed during the entire treatment-period. The total duration of treatment was 1 year and 3 months. This individualised homoeopathic treatment resulted in complete resolution of all presenting complaints [Table 1] which were also supported by post-treatment ultrasonography (USG)-findings [Figure 2]. The case was kept under observation for another 6 months, during which none of the symptoms recurred.
| Date of visit | Symptoms | Medicine with doses and repetition | Justification of the medicine and potency |
|---|---|---|---|
| 01 May 2021 | LMP 17 April 2021 Pain during menses was better than before, but bleeding remained the same. White discharge per vagina increased for 7 days after taking medicine and then reduced considerably (almost 60% better) Sleep improved. Forgetfulness was as before. |
Placebo for 30 days | Gradual improvement of the patient in all parameters precluded any repetition. |
| 05 June 2021 | LMP 20 May 2021 Pain and heavy bleeding during menstruation were reduced significantly. During her LMP, the patient required 14 sanitary pads. (Previously, it was approximately 20). White discharge per vagina was almost resolved. Patient had a sound sleep for 5–6 hours. Forgetfulness reduced. |
-Same- | -Same- |
| 07 July 2021 | LMP 18 June 2021 Pain and bleeding remained the same as that of previous menstrual period. White discharge per vagina-same as before. There was no disturbance in sleep. Memory improved. |
Medorrhinum 200/1 dose in 10 mL water | After a period of significant improvement, the case came to a standstill condition, which demanded repetition of the same medicine with the same potency. |
| 10 August 2021 | LMP 24 July 2021 Pain during LMP reduced considerably. The amount of menstrual bleeding was reduced. Patient required 10–12 sanitary pads during her LMP. There was a marked reduction in white discharge per vagina. Memory for the recent past was intact. |
Placebo | There was noticeable reduction in the intensity of symptoms after repetition of the remedy. Therefore, placebo was prescribed. |
| 15 September 2021 | LMP 30 August 2021 Pain and bleeding during LMP were better than before. For the past 5 days the patient developed a mild asthmatic attack. The dyspnoea aggravated at night compelling the patient to wake up. |
Placebo | Reappearance of old symptoms indicates good prognosis of the case. As dyspnoea was not severe one, no medicine was prescribed and waited for spontaneous resolution. |
| 01 October 2021 | Menstrual complaints were as before. Pain had reduced compared to previous visits, but deep pain was still persisting. Breathing distress was persistent with gradually increasing intensity. |
Medorrhinum 1 M/1 dose Once daily for 1 day |
As the symptom complex came to a static condition after a period of improvement and old symptoms failed to resolve spontaneously, a higher potency of the medicine was prescribed. |
| 25 November 2021 | There was marked relief in all symptoms. Dyspnoea almost resolved. Menstrual complaints and white discharge per vagina reduced significantly. |
Placebo | Improvement of the patient in all parameters contraindicated any repetition |
| 05 January 2022 | LMP 25 December 2021 Pain during menstruation became very mild. Menstrual bleeding came to normal as regard to its quantity. There has been no attack of dyspnoea since the past 30 days. |
Placebo | -Same- |
| 20 March 2022 | No residual symptom. | Placebo Advice for USG of lower abdomen. |
-Same- |
| 13 May 2022 | All complaints resolved. BPE showed no abnormality. | Placebo | -Same- USG of lower abdomen dated 11 May 2022 revealed normal study with mild collection of fluid in Pouch of Douglas. |
BPE: Bimanual pelvic examination, LMP: Last menstrual period, USG: Ultrasonography
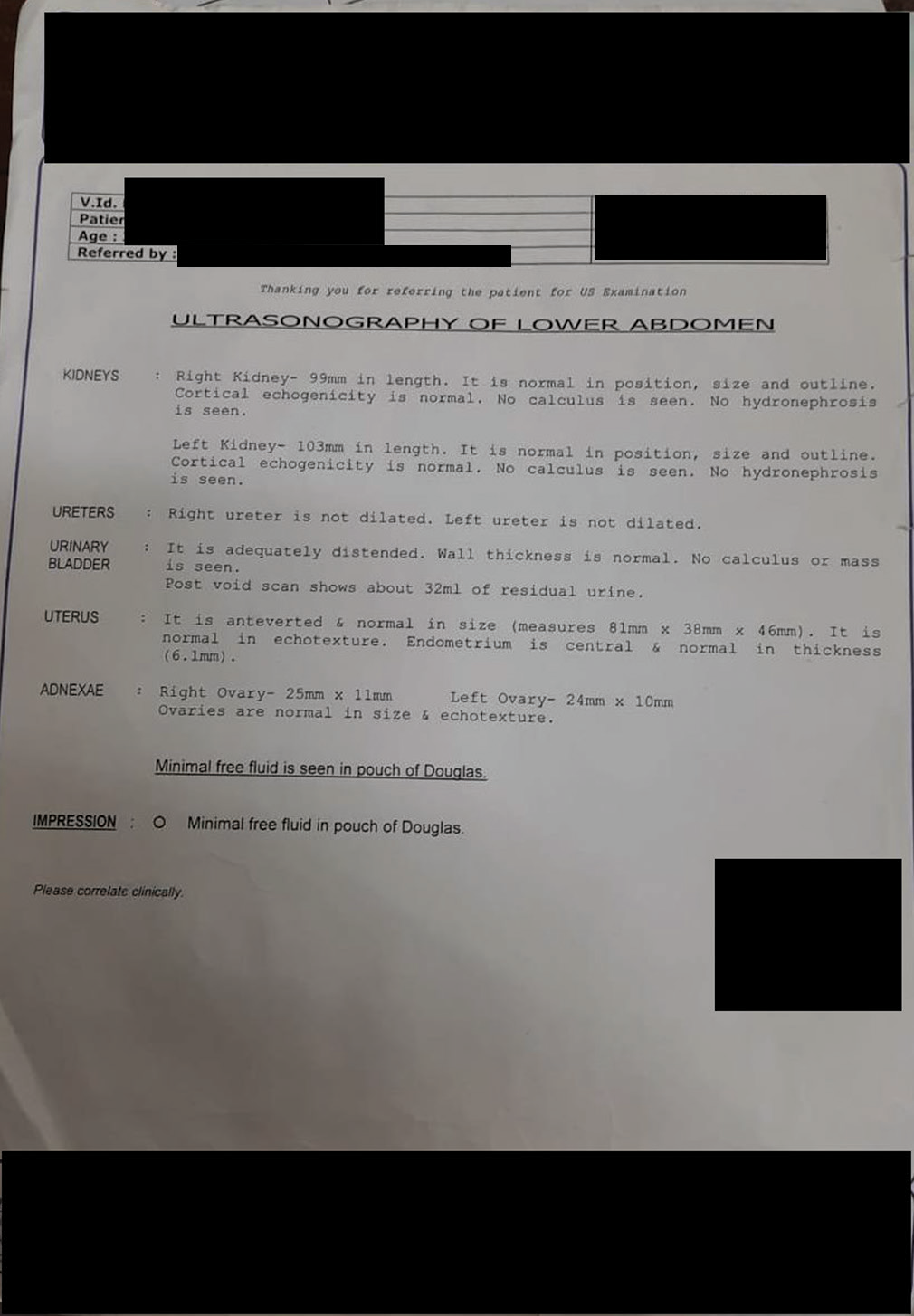
- After treatment
DISCUSSION
Adenomyosis is a uterine condition where the endometrial glands and stroma are pathologically demonstrated in the uterine myometrium layer which is a distinct entity of polyp; adenomyosis; leiomyoma; malignancy and hyperplasia; coagulopathy; ovulatory dysfunction; endometrial; iatrogenic and not yet classified – International Federation of Gynaecology and Obstetrics classification of aetiological factors of abnormal uterine bleeding.[17] As there are significant limitations in conventional medicine which includes higher rate of recurrences, adverse effects of oral analgesics and inability to resolve the disorder without surgical intervention and hysterectomy is mostly advised treatment modality, an alternative approach is warranted to preserve the uterus.
After extensive searches in different databases, some cases were found to provide evidence of homoeopathy enabling successful treatment of adenomyosis. Ponnam et al. successfully treated a case of adenomyosis in a perimenopausal woman using conium maculatum following individualisation and constitutional approach.[18] Another case study by the same author showed symptomatic relief and complete cure of adenomyosis in a 27-year-old woman, with Trillium pendulum 30, Natrum Muriaticum 30 and Natrum Muriaticum 200 prescribed at different time points as suggested by the existing symptom totality.[19]
In the past decade, the incidence of adenomyosis in young fertile women has been found to be significantly high.[3] The case was approached through meticulous homoeopathic case taking, identifying the uncommon peculiars and strict individualisation through totality of characteristic symptoms. The symptom totality and family background of sycotic miasm clearly indicated Medorrhinum, an antisycotic remedy which was prescribed in higher dilutions and minimum dose to avoid any unwanted aggravations. The medicine was repeated as required. The outcome was complete resolution of entire signs and symptoms which were supported by the post-treatment USG report.
In this case study, a young multiparous woman presented with profuse menstrual bleeding which is the most common presentation of adenomyosis as described in Stewart’s classification system[20] and appeared to be a challenge to homoeopathy as she had undergone all available treatments which had yielded no results. In this particular case, we faced several difficulties regarding therapeutic approach and management. As the patient presented with heavy protracted bleeding with severe dysmenorrhoea, our medical team was also anxious about the clinical outcome of the case. We maintained a strong conviction regarding the homoeopathic single medication and its principles; the outcome became obvious in subsequent visits. Through homoeopathy, we could improve the patient’s quality of life in terms of subjective symptoms such as pain, bloated feeling, menorrhagia and preserve the uterus. Thus, homoeopathy may help women with this condition. The modified Naranjo criteria score after the treatment was 10 which exclusively showed positive causal attribution of the individualized Homoeopathic medicine in this case [Table 2].[21] Nevertheless, a single case report cannot proclaim the treatment efficacy of homoeopathy in adenomyosis. To produce strong evidence, a large-scale randomised controlled trial with sound methodology is suggested.
| Domains | Yes | No | Not sure or N/A |
|---|---|---|---|
| 1. Was there an improvement in the main symptom or condition for which the homoeopathic medicine was prescribed? | +2 | 0 | 0 |
| 2. Did the clinical improvement occur within a plausible time frame relative to the drug intake? | +1 | 0 | 0 |
| 3. Was there an initial aggravation of symptoms? | +1 | 0 | 0 |
| 4. Did the effect encompass more than the main symptom or condition (i.e. were other symptoms ultimately improved or changed)? | +1 | 0 | 0 |
| 5. Did overall well-being improve? | +1 | 0 | 0 |
| 6. Did the course of improvement follow Hering’s Rule? | 0 | 0 | 0 |
| 7. Did ‘old symptoms’ (defined as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? | +1 | 0 | 0 |
| 8. Are there alternate causes (other than the medicine) that – with a high probability – could have caused the improvement? (known course of disease, other forms of treatment and other clinically relevant interventions) | 0 | +1 | 0 |
| 9. Was the health improvement confirmed by clinical observation? | +2 | 0 | 0 |
| 10. Did repeat dosing, if conducted, create similar clinical improvement? | 0 | 0 | 0 |
| Total score | 10 | ||
N/A: Not applicable
CONCLUSION
In the present day, the incidence of adenomyosis and its complicated forms (mostly with endometriosis) are gradually increasing. Due to limited treatment options in conventional medicine, an alternative approach is necessary. This case report highlights a successful instance of cure of adenomyosis through long-term homoeopathic therapy which was solely based on the totality of symptoms. The positive outcomes evident in this case underscore the potential of homoeopathy as an alternative for successfully treating adenomyosis.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- The history of endometriosis. Gynecol Obstet Invest. 2014;78:1-9.
- [CrossRef] [PubMed] [Google Scholar]
- Recent advances in understanding and managing adenomyosis. F1000Res. 2019;8:F1000. Faculty Rev-283
- [CrossRef] [PubMed] [Google Scholar]
- Transvaginal sonographic features of diffuse adenomyosis in 18-30 year old nulligravid women without endometriosis: Association with symptoms. Ultrasound Obstet Gynecol. 2015;46:730-6.
- [CrossRef] [PubMed] [Google Scholar]
- Pathogenesis of adenomyosis: An update on molecular mechanisms. Reprod Biomed Online. 2017;35:592-601.
- [CrossRef] [PubMed] [Google Scholar]
- Myostatin, follistatin and activin type II receptors are highly expressed in adenomyosis. Fertil Steril. 2015;104:744-52.e1.
- [CrossRef] [PubMed] [Google Scholar]
- Adenomyosis: Review of the literature. J Minim Invasive Gynecol. 2011;18:428-37.
- [CrossRef] [PubMed] [Google Scholar]
- Adenomyosis: Current perspectives. Obstet Gynecol Clin North Am. 1989;16:221-35.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence and risk factors of adenomyosis at hysterectomy. Hum Reprod. 2001;16:2418-21.
- [CrossRef] [PubMed] [Google Scholar]
- Symptoms and classification of uterine adenomyosis, including the place of hysteroscopy in diagnosis. Fertil Steril. 2018;109:380-8.e1.
- [CrossRef] [PubMed] [Google Scholar]
- Adenomyosis: A clinical review of a challenging gynecologic condition. J Minim Invasive Gynecol. 2016;23:164-85.
- [CrossRef] [PubMed] [Google Scholar]
- Magnetic resonance imaging and transvaginal ultrasonography for the diagnosis of adenomyosis. Fertil Steril. 2001;76:588-94.
- [CrossRef] [PubMed] [Google Scholar]
- Adenomyosis: A systematic review of medical treatment. Gynecol Endocrinol. 2016;32:696-700.
- [CrossRef] [PubMed] [Google Scholar]
- Management of uterine adenomyosis: Current trends and uterine artery embolization as a potential alternative to hysterectomy. Insights Imaging. 2019;10:48.
- [CrossRef] [PubMed] [Google Scholar]
- Pocket manual of homoeopathic materia medica and repertory (9th ed). New Delhi: B. Jain Publishers; 2016. p. :414-7.
- [Google Scholar]
- FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in non-gravid women of reproductive age. Int J Gynecol Obstet. 2011;113:3-13.
- [CrossRef] [PubMed] [Google Scholar]
- Adenomyosis in a perimenopausal woman treated by potentized poison hemlock-a case report. Homœopathic Links. 2019;32:251-5.
- [CrossRef] [Google Scholar]
- Evaluation of the modified naranjo criteria for assessing causal attribution of clinical outcome to homeopathic intervention as presented in case reports. Homeopathy. 2020;109:191-7.
- [CrossRef] [PubMed] [Google Scholar]




