
Translate this page into:
Cordyceps sinensis 30c and Achyranthes aspera ointment in the treatment of molluscum contagiosum: A case series investigation
*Corresponding author: Dr. Vettrivel Arul, Department of Community Medicine, Vinayaka Mission’s Homoeopathic Medical College and Hospital, Vinayaka Mission’s Research Foundation (DU), Salem, Tamil Nadu, India. veldoc4565@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Arul V. Cordyceps sinensis 30C and Achyranthes aspera ointment in the treatment of molluscum contagiosum: A case series investigation. J Intgr Stand Homoeopathy. 2024;7:107-14. doi: 10.25259/JISH_64_2023
Abstract
This study explores the effectiveness of a novel approach using a combination of Cordyceps sinensis 30C and topical Achyranthes aspera ointment in treating Molluscum contagiosum. The ointment was formulated by blending Achyranthes aspera Q with petrolatum, following standardized procedures. Two cases of Molluscum contagiosum were treated internally with Cordyceps sinensis 30C and externally with the Achyranthes aspera ointment. Treatment progress was closely monitored, and the modified Naranjo criteria were applied to assess the causal relationship between the treatment and clinical outcomes. Both cases showed significant improvement, with lesions disappearing within three months. The Naranjo scores indicated a potential causal link between the treatment and the observed outcomes. This combined approach offers a promising alternative in homoeopathy for managing Molluscum contagiosum, though further research and larger clinical trials are necessary to confirm its efficacy and safety. The integration of external applications in homoeopathy remains a subject of debate, yet this approach aligns with evidence-based practices, potentially improving patient care.
Keywords
Achyranthes aspera
Antiviral treatment
Cordyceps sinensis
Homoeopathy
Molluscum contagiosum

INTRODUCTION
Molluscum contagiosum, also known as water warts, is a benign skin condition caused by the Molluscum contagiosum virus (MCV), a member of the Poxviridae family.[1] MCV is primarily transmitted through direct contact with infected skin, which can occur through sexual, non-sexual, or autoinoculation routes.[2] The skin manifestations of this condition are referred to as Mollusca. These typical lesions appear as dome-shaped, round, pinkish-purple growths with a shiny and dimpled centre.[3] The incubation period for molluscum contagiosum can range from 2 weeks to 6 months.[4] It is important to note that the virus infects only keratinocytes and remains confined to the epidermis without systemic spread.[5] MCV produces proteins that inhibit the human antiviral immune response, leading to the persistence of skin lesions.[6] The duration of these lesions varies, but in most cases, they resolve spontaneously within 6–9 months.[7] The size, shape, and location of the lesions can vary, with more variability observed in immunosuppressed individuals.[8] Diagnosis is primarily based on clinical examination, with dermoscopy being a valuable clinical tool. In cases of diagnostic uncertainty, confocal microscopy or skin biopsy may be considered.[9] The necessity for active treatment of Molluscum contagiosum remains a topic of debate;[10] however, consensus suggests that treatment should be considered in cases of extensive disease, complications, or aesthetic concerns. Various treatment options are available, including mechanical, chemical, immunomodulatory, and antiviral approaches. Mechanical methods encompass cryotherapy (freezing the lesions), curettage (physical removal), and pulse dye laser therapy. Chemical treatments involve agents such as cantharidine (blister-inducing) and potassium hydroxide (keratin dissolution), among others. Immunomodulatory strategies include imiquimod and other methods such as oral cimetidine, interferon alfa, candidin, and diphencyprone. Severe cases may require antiviral agents such as cidofovir.[11] In addition, emerging therapies include topical sinecatechins, intralesional 5-fluorouracil, hyperthermia, and Zoster Immune Globulin.[12] These treatment modalities offer a range of options for managing molluscum contagiosum, depending on the specific clinical situation.
Cordyceps sinensis, an extraordinary medicinal fungus, has captured the attention of researchers and medical practitioners due to its remarkable antiviral properties. Scientific investigations have provided compelling evidence that C. sinensis can effectively combat a wide range of viruses through diverse mechanisms. In the realm of homoeopathic medicine, Cordyceps is utilised to address a wide spectrum of health issues, such as fatigue, respiratory problems, sexual dysfunction, and skin-related concerns. Cordyceps also fortifies the body’s defenses against a broad spectrum of pathogenic microorganisms, including bacteria, fungi, and viruses.[13] Cordycepin, a component of C. sinensis, has been identified as a potent antiviral agent with significant therapeutic potential.[14] One of the most intriguing findings is related to its activity against novel coronaviruses, including those responsible for the COVID-19 pandemic. Molecular dynamics simulations have offered valuable insights into the interaction between cordycepin and the receptor-binding domain (RBD) of the spike protein present in these coronaviruses. This interaction is crucial, as it suggests that cordycepin can serve as a pan-coronavirus fusion inhibitor. By strongly binding to the spike protein’s RBD, cordycepin has the potential to prevent viral particles from entering and infecting host cells. This discovery represents a promising avenue for developing treatments against coronaviruses.[15] C. sinensis also demonstrates its effectiveness against other viral infections. For instance, studies have shown that C. sinensis extract can reduce viral titers and enhance the immune response in mice infected with the H1N1 influenza virus. This demonstrates its efficacy in combating influenza infections by both reducing viral replication and boosting the body’s immune defenses.[16] Furthermore, C. sinensis has shown promise in inhibiting the replication of the hepatitis B virus, which is notorious for its persistence and resistance to treatment. This suggests that C. sinensis could offer valuable therapeutic options for individuals suffering from challenging hepatitis B infections.[17] Cordycepin demonstrates a robust ability to hinder the replication of poxviruses, particularly by significantly reducing the production of cytoplasmic viral RNA and poly(A) (by more than 94% at 40 µg/mL) within cells infected by the vaccinia virus, a member of the Poxviridae family.[18] The antiviral potential of cordycepin extends beyond these examples, as various research groups have reported its activity against a wide spectrum of viruses. This includes influenza virus, plant viruses, human immunodeficiency virus, murine leukaemia virus, and Epstein–Barr virus (EBV), among others.[19] These findings collectively highlight C. sinensis as a promising natural source for combating a diverse array of viral pathogens.
Shifting our focus to Achyranthes aspera Linn, commonly known as Apamarga, this plant has a rich tradition of use in Tamil Nadu, India, for treating cuts and wounds. In scientific studies, researchers prepared ethanol and aqueous extracts from the leaves of A. aspera and assessed their wound healing and antioxidant properties using well-established models. The results of these investigations provided strong evidence of A. aspera’s ability to promote wound healing and exhibit potent antioxidant properties. These properties are crucial in facilitating the repair of damaged tissues and preventing the harmful effects of free radicals, which can hinder the healing process.[20] In addition, A. aspera has exhibited significant anti-cancer potential in studies focusing on its methanol leaf extract. Researchers observed its ability to inhibit the EBV early antigen induced by the tumour promoter 12-O-tetradecanoylphorbol-13-acetate, in Raji cells.[21] Furthermore, in a mouse skin carcinogenesis test, the total methanol extract of A. aspera demonstrated a pronounced anticarcinogenic effect.[22] This suggests that A. aspera holds promise in preventing or inhibiting the development of skin cancer, a condition with substantial health implications. Interestingly, traditional Ayurvedic practices have employed A. aspera in the form of an aqueous solution (alkaline ash) for intralesional infiltration as a method for wart removal.[23] Within the domain of homoeopathy, A. Aspera (Achy-a.) is employed to address a range of skin conditions characterised by erythematous, vesicular, papular, and pustular lesions typically affecting the hands and feet. These conditions frequently manifest with malodorous discharges and find application in treating ailments such as carbuncles, folliculitis, eczematous dermatitis, pyoderma, light eruptions, and systemic lupus erythematosus.[24] This highlights the plant’s historical use in addressing viral-induced skin conditions, aligning with its modern scientific evaluation as a potential antiviral agent.
In the context of treating molluscum contagiosum, two distinct approaches are mentioned. First, C. sinensis 30C, available in homoeopathic dilution, is administered internally. This choice is informed by the fungus’s well-documented antiviral properties and its ability to activate the immune system. By taking C. sinensis internally it is believed to assist in combating the viral infection and supporting the body’s natural defenses. The selection of 30C potency is rooted in the notion that C. sinensis 30C exhibits superior antioxidant activity compared to lower potencies. The antioxidant activity of a drug can potentially enhance its antiviral properties, making it a preferable option for this purpose.[25,26] Second, A. aspera Q, available as a homoeopathic mother tincture, is used to formulate a homoeopathic ointment with petrolatum as a vehicle using the fusion method according to Homoeopathic Pharmcopoeia of India (HPI) guidelines.[27] This external application leverages A. Aspera’s recognised antiviral properties, making it effective for the removal of warts in traditional medicine. The combined approach of internal administration and topical application reflects a scientific strategy for managing molluscum contagiosum by harnessing the antiviral potential of these natural substances.
Process of study
In both cases, symptoms were meticulously examined, diagnoses were accurately confirmed, and prescriptions were formulated based on careful pathological assessment with homoeopathic medications. These cases were meticulously documented and presented following their successful resolution.
Study design
This was a clinical case study.
Inclusion criteria
Individuals with a verified diagnosis of Molluscum contagiosum who willingly provided informed consent and committed to regular follow-up evaluations to track their treatment progress and outcomes were included in the study.
Exclusion criteria
Individuals with a confirmed diagnosis of Molluscum contagiosum who had a history of severe allergies or adverse reactions to the prescribed homoeopathic medications, as well as those who were unable or unwilling to adhere to the recommended treatment regimen and follow-up assessments. In addition, patients with other pre-existing skin conditions or medical issues that could substantially affect the assessment of Molluscum contagiosum treatment outcomes were excluded from the study.
Materials
C. sinensis 30C was obtained from Helios Pharmacy in the United Kingdom, and A. aspera Q was sourced from a reputable homoeopathic manufacturer with Good Manufacturing Practices certification. Petrolatum (Vaseline) was purchased from Mercury’s Scientific Chemicals Industries in Salem, Tamil Nadu.
Method
Preparation of A. aspera ointment
The methodology employed according to HPI guidelines,[27] the process begins by melting Vaseline in a water bath to prevent the material from being subjected to excessively high temperatures. This melting process starts with the substance having the highest melting point and gradually incorporates A. aspera Q, following a descending order based on their respective melting points. Furthermore, the formulation of medicated ointments adheres to a standardised procedure. This entails combining the mother tincture of the desired drug with a suitable base. Specifically, for this particular formulation, a ratio of 1 part A. aspera Q is blended with nine parts of the base.
CASE SERIES
The case series involves two instances in which individuals were diagnosed with and displayed symptoms of Molluscum contagiosum. The diagnosis of Molluscum contagiosum was based on the presence of raised, pearly white, and dome-shaped skin eruptions on their faces.
In treating Molluscum contagiosum, a novel method was employed, which integrates the antiviral attributes of C. sinensis and A. aspera. C. sinensis, renowned for its potent antiviral component called cordycepin, was administered in a homoeopathic dilution to stimulate the immune system and effectively combat various viral infections, including novel coronaviruses. Simultaneously, A. aspera, known for its wound-healing and antioxidant properties, was applied topically in the form of a homoeopathic ointment. This topical intervention facilitated the removal of warts and the management of skin conditions associated with Molluscum contagiosum. This two-pronged method harnesses the antiviral potential of these natural substances, providing a scientific strategy for addressing Molluscum contagiosum.
To determine whether the observed clinical improvement could be attributed to the prescribed treatment, the modified Naranjo criteria assessment tool was utilised. Consent for the anonymous publication of these cases was obtained from the parents in the case of minors. The reporting of these cases adheres to the HOM-CASE guideline, which extends from the CARE guidelines and ensures comprehensive reporting of medical cases.
Case 1
Patient information
A school-going girl aged 6 years of Indian ethnicity.
Main symptoms
The patient, aged about 6 years, belonging to a middle socioeconomic family, presented to the clinic on 4 February 2022 with eruptions with itching on the chin and under the lips, pearly white in appearance for the past 2 months, gradually increasing in number.
History of present complaint
The patient received conventional medications, such as lidocaine ointment and cantharidin, to address the eruptions for a duration of 1 month. However, there was no observable improvement, and the eruptions began to progressively spread to nearby area.
Local examination
Location
Beneath the lower lip and on the chin.
Number and size of eruptions
Approximately 15–20, measuring 0.5–2 mm each.
Pattern of distribution and arrangement
Displaying an irregular, asymmetrical layout.
Character
These papules are characterised as a firm, ranging from white to flesh-coloured, and exhibit a dome-shaped appearance with a central depression, resembling pearly papules.
Prescription
C. sinensis 30C was administered internally as three pills 3 times a day for 1 month, while externally, A. aspera ointment was prescribed for application twice daily over the same 1-month period. This treatment plan was determined based on a thorough assessment of the patient’s pathology.
The case was monitored monthly, revealing a significant decrease in the size of the eruptions. After 3 months, there were no remaining traces of the eruptions [Table 1 and Figure 1]. The patient’s modified Naranjo criteria total score was +9/13, indicating that the improvement in the patient’s condition could be attributed to C. sinensis 30C and A. aspera [Table 2]. Subsequently, the patient continued to be monitored for an additional 6 months, and there were no signs of a recurrence of the initial complaints.

- (a) Before treatment. (b) After treatment.
| Date | Symptoms | Prescription |
|---|---|---|
| March 03, 2022 | A minor decrease in the dimensions of Molluscum contagiosum lesions. | C. sinensis 30C: 3 pills, thrice daily, A. aspera ointment: Apply externally twice daily |
| April 07, 2022 | A continued decrease in the size of Molluscum contagiosum lesions has been noted. | C. sinensis 30C: 3 pills, twice daily, A. aspera ointment: Apply externally twice daily |
| May 02, 2022 | Nearly all of the existing Molluscum contagiosum eruptions were observed to have cleared, with no new eruptions reported. | Placebo 3 pills, thrice daily, A. aspera ointment: Apply externally twice daily |
| June 10, 2022 | There have been no fresh Molluscum contagiosum eruptions. | Placebo 3 pills, thrice daily |
| November 10, 2022 | There has been no reappearance of previous lesions nor the development of new Molluscum contagiosum eruptions. | The treatment was discontinued, and the patient reported to provide feedback for 6 months. |
C. sinensis:Cordyceps sinensis, A. aspera: Achyranthes aspera
| S. No. | Modified Naranjo criteria | Yes | No | Not sure | Case 1 | Case 2 |
|---|---|---|---|---|---|---|
| 1. | Was there an improvement in the main symptom or condition for which the homoeopathic medicine was prescribed? | +2 | −1 | 0 | +2 | +2 |
| 2. | Did the clinical improvement occur within a plausible timeframe relative to the drug intake? | +1 | −1 | 0 | +1 | +1 |
| 3. | Was there an initial aggravation of symptoms? | 0 | 0 | 0 | 0 | 0 |
| 4. | Did the effect encompass more than the main symptom or condition (i.e., were other symptoms ultimately improved or changed)? | +1 | 0 | 0 | +1 | +1 |
| 5. | Did overall well-being improve? (suggest using a validated scale) | +1 | 0 | 0 | +1 | +1 |
| 6. | Direction of cure: did some symptoms improve in the opposite order of the development of symptoms of the disease? | 0 | 0 | 0 | 0 | 0 |
| The direction of cure: did at least two of the following aspects apply to the order of improvement of symptoms —from organs of more importance to those of less importance – from deeper to more superficial aspects of the individual – from the top downward? | +1 | 0 | 0 | +1 | +1 | |
| 7. | Did old symptoms (defined as nonseasonal and non-cyclical that were previously thought to have resolved) reappear temporarily during the course of improvements? | 0 | 0 | 0 | 0 | 0 |
| 8. | Are there alternate causes (other than the medicine) that – with a high probability – could have caused the improvement? (Consider the known course of the disease, other forms of treatment, and other clinically relevant interventions). | −3 | +1 | 0 | +1 | +1 |
| 9. | Was the health improvement confirmed by any objective evidence? (e.g., lab test, clinical observation, etc.) | +2 | 0 | 0 | +2 | +2 |
| 10. | Did repeat dosing, if conducted, create similar clinical improvement? | 0 | 0 | 0 | 0 | 0 |
| Total score (Maximum score= +13; Minimum score = −3) | +9 | +9 |
Case 2
Patient information
A baby boy aged 9 months of Indian ethnicity.
Main symptoms
On 7 July 2022, a 9-month-old patient originating from a low socioeconomic background, presented at the clinic with a facial eruption. These eruptions exhibited a reddish-pink, semi-transparent appearance and were characterised by umbilicated papules. This condition had persisted for the preceding 3 months, during which time it displayed a gradual increase in both size and quantity. Notably, the papules were non-tender and displayed a soft consistency.
History of present complaint
The patient had not taken any treatment previously.
Local examination
Location
All over the face, dominantly near the eyes.
Number and size of eruptions
Approximately 20–30, measuring 0.5–3.5 mm each.
Pattern of distribution and arrangement
Displaying an irregular, asymmetrical layout.
Character
These eruptions presented with a reddish-pink, semi-translucent appearance and were typified by the presence of umbilicated papules.
Prescription
Internally, C. sinensis 30C was administered in the form of three pills thrice daily for a duration of 1 month. In addition, externally, A. aspera ointment was prescribed to be applied twice daily for the same 1-month period. This prescription was made based on pathological considerations.
Follow-up assessments were conducted on a monthly basis, revealing a notable reduction in the size of the eruptions. After 3 months, no evidence of eruptions remained [Table 3 and Figure 2]. The patient’s modified Naranjo criteria total score was +9/13, suggesting that C. sinensis 30C and A. aspera may have contributed to the patient’s improvement [Table 2]. Further, follow-up over the course of 6 months showed no recurrence of the initial complaints in this patient.
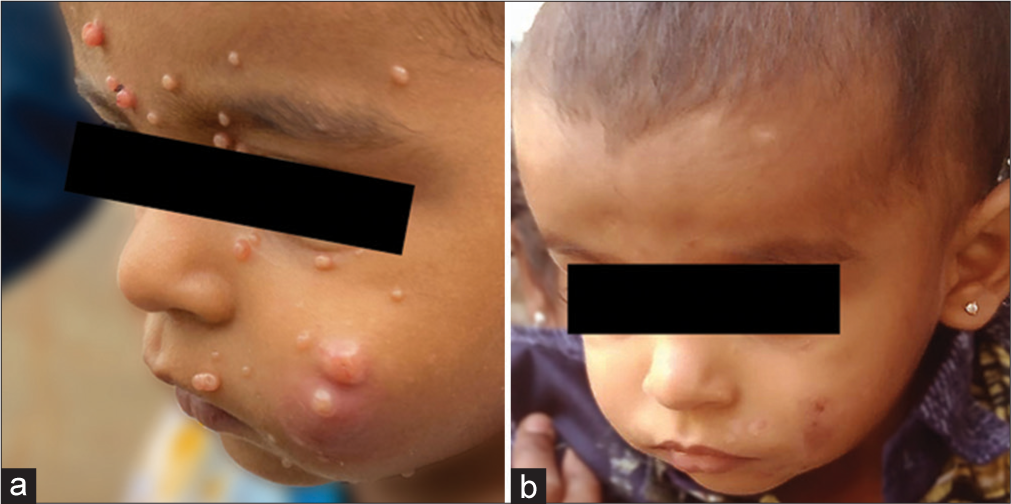
- (a) Before treatment. (b) After treatment.
| Date | Symptoms | Prescription |
|---|---|---|
| August 08, 2022 | A decrease in the size of the Molluscum contagiosum lesions was noted. | C. sinensis 30C: 3 pills, thrice daily, A. aspera ointment: Apply externally twice daily |
| September 10, 2022 | A continued decrease in the size of Molluscum contagiosum lesions has been noted. | C. sinensis 30C: 3 pills, twice daily, A. aspera ointment: Apply externally twice daily |
| October 05, 2022 | Nearly all of the Molluscum contagiosum eruptions vanished, leaving only a faint discoloration. | Placebo 3 pills, thrice daily, A. aspera ointment: Apply externally twice daily |
| November 01, 2022 | No new Molluscum contagiosum eruptions have occurred; however, there is some slight discoloration present. | Placebo 3 pills, thrice daily |
| July 06, 2023 | There has been no reappearance of previous lesions nor the development of new Molluscum contagiosum eruptions. | The treatment was discontinued, and the patient reported to provide feedback for 6 months. |
C. sinensis:Cordyceps sinensis, A. aspera: Achyranthes aspera
RESULTS
In this case series, two cases of Molluscum contagiosum were treated with a combination of C. sinensis 30C and topical A. aspera ointment. Both cases showed significant clinical improvement, as evidenced by a modified Naranjo criteria score of +9/13, suggesting a potential causal relationship between the treatment and the observed outcomes. The introduction of this novel approach using C. sinensis and A. aspera presents a promising alternative for managing this viral skin condition.
DISCUSSION
The case series introduces a novel approach to treating Molluscum contagiosum by combining the antiviral properties of C. sinensis and A. aspera through internal administration and topical application, resulting in significant clinical improvement in two cases. However, the limited sample size highlights the need for further research and clinical trials to validate the treatment’s efficacy and safety. The historical contradiction regarding external application in homoeopathy, as seen in the differences between the 5th and 6th editions of the Organon of Medicine, complicates the discussion, but ongoing clinical trials and recent advancements in homoeopathy suggest that external applications can serve as valuable adjuvants in treatment, even when different medicines are used internally and externally. This evidence-based approach has the potential to empower clinicians to make more informed decisions for patient care, potentially leading to improved outcomes, particularly in cases where conventional treatments are ineffective or undesirable.
CONCLUSION
This innovative treatment approach for Molluscum contagiosum, leveraging C. sinensis and A. aspera’s antiviral properties, holds promise in homoeopathy’s role in dermatology. While initial results are promising, further research, larger patient cohorts, and rigorous clinical trials are essential for establishing its efficacy and safety. The historical debate on external applications in homoeopathy adds complexity to this emerging practice. Yet, as medicine embraces evidence-based strategies and novel therapies, this approach offers hope for those with Molluscum contagiosum, presenting new treatment possibilities and the potential for enhanced patient care.
Acknowledgements
I extend my sincere gratitude to Dr. Mary Adharshna for her assistance in manuscript writing. I also appreciate the patients and VeVe Pharmacy for their invaluable contributions, enabling the successful execution of this study.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that they have used artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript or image creations.
Financial support and sponsorship
Nil.
References
- Molluscum-contagiosum-virus in einer epidermalzyste. J Dtsch Dermatol Ges. 2018;16:1144-6.
- [CrossRef] [PubMed] [Google Scholar]
- Molluscum contagiosum: An update and review of new perspectives in etiology, diagnosis, and treatment. Clin Cosmet Investig Dermatol. 2019;12:373-81.
- [CrossRef] [PubMed] [Google Scholar]
- Dermatoscopy in inflammatory and infectious skin disorders. G Ital Dermatol Venereol. 2015;150:521-31.
- [Google Scholar]
- Expanding the morphologic heterogeneity of stromal changes in molluscum contagiosum infection. Am J Dermatopathol. 2018;40:941-3.
- [CrossRef] [PubMed] [Google Scholar]
- Molluscum contagiosum virus protein MC005 inhibits NF-κB activation by targeting NEMO-regulated IκB kinase activation. J Virol. 2017;91:e00545-17.
- [CrossRef] [PubMed] [Google Scholar]
- Epidermal growths In: Lookingbill and marks' principles of dermatology (6th ed). London: Elsevier; 2019. p. :41-61. Ch. 5
- [CrossRef] [Google Scholar]
- Dermatologic manifestations of HIV infection In: Cohen J, Opal SM, Powderly WG, eds. Infectious diseases (3rd ed). London: Mosby; 2010. p. :994-1001. Ch. 95
- [CrossRef] [Google Scholar]
- Clinical and dermoscopic overlap of genital molluscum contagiosum with condyloma acuminate. SAGE Open Med Case Rep. 2022;10:2050313X221086100.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of molluscum contagiosum in adult, pediatric, and immunodeficient populations. J Cutan Med Surg. 2014;18:299-306.
- [CrossRef] [PubMed] [Google Scholar]
- 2020 European guideline on the management of genital molluscum contagiosum. J Eur Acad Dermatol Venereol. 2021;35:17-26.
- [CrossRef] [PubMed] [Google Scholar]
- Recalcitrant molluscum contagiosum successfully treated with sinecatechins. Dermatol Ther. 2016;29:217-8.
- [CrossRef] [PubMed] [Google Scholar]
- A concise review of mushrooms antiviral and immunomodulatory properties that may combat against COVID-19. Food Chem Adv. 2022;1:100023.
- [CrossRef] [PubMed] [Google Scholar]
- Medicinal fungi with antiviral effect. Molecules. 2022;27:4457.
- [CrossRef] [PubMed] [Google Scholar]
- Novel fatty acid in Cordyceps suppresses influenza A (H1N1) virus-induced proinflammatory response through regulating innate signaling pathways. ACS Omega. 2021;6:1505-15.
- [CrossRef] [PubMed] [Google Scholar]
- Cordyceps sinensis attenuates HBx-induced cell apoptosis in HK-2 cells through suppressing the PI3K/Akt pathway. Int J Mol Med. 2020;45:1261-9.
- [CrossRef] [PubMed] [Google Scholar]
- Inhibition of host protein synthesis in vaccinia virus-infected cells in the presence of cordycepin (3'-deoxyadenosine) J Virol. 1978;25:11-8.
- [CrossRef] [PubMed] [Google Scholar]
- Cordycepin is a novel chemical suppressor of Epstein-Barr virus replication. Oncoscience. 2014;1:866-81.
- [CrossRef] [PubMed] [Google Scholar]
- Wound healing and antioxidant activity of Achyranthes aspera. Pharm Biol. 2008;46:824-8.
- [CrossRef] [Google Scholar]
- Cancer chemopreventive activity of Achyranthes aspera leaves on Epstein-Barr virus activation and two-stage mouse skin carcinogenesis. Cancer Lett. 2002;177:1-5.
- [CrossRef] [PubMed] [Google Scholar]
- The potent plant for traditional medicine system: “Achyranthes aspera”. Int J Drug Dev Res. 2021;13:157.
- [Google Scholar]
- Subcutaneous intralesional Ksharodaka injection: A novel treatment for the management of Warts: A case series. J Ayurveda Integr Med. 2014;5:236-40.
- [CrossRef] [PubMed] [Google Scholar]
- Antioxidant and cytotoxic potential of potentized preparation of Cordyceps sinensis in vitro in cancer cell lines. Indian J Res Homoeopathy. 2023;17:2.
- [CrossRef] [Google Scholar]
- Antioxidant potential of antiviral drug umifenovir. Molecules. 2020;25:1577.
- [CrossRef] [PubMed] [Google Scholar]
- Homoeopathic pharmacopoeia of India (H.P.I) (1st ed). New Delhi: Controller of Publications; 1971.
- [Google Scholar]




