
Translate this page into:
Homoeopathic management of pituitary macroadenoma: A case report
*Corresponding author: Dr. Pralay Sharma, National Institute of Homoeopathy, Kolkata, West Bengal, India. pralaysharma68@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sharma P, Parveen S. Homoeopathic management of pituitary macroadenoma: A case report. J Intgr Stand Homoeopathy. 2024;7:83-8. doi: 10.25259/JISH_37_2023
Abstract
Pituitary adenomas (PAs) are usually slow growing and non-malignant, but place a heavy burden on patients and health-care systems. The estimated worldwide prevalence of PAs is 17%. Trans-sphenoidal surgical adenoma resection is the initial treatment chosen for all tumours except prolactinomas. Radiation is reserved for patients in whom tumour size, hormone levels or both cannot be adequately reduced after surgery, drug therapy or both. There are published case reports showing promising results in PAs treated with homoeopathy. This paper describes a case on pituitary macroadenoma successfully treated with a single homoeopathic medicine, following the basic principles of homoeopathy. The case was repertorised using O. E. Boericke’s repertory to select the homoeopathic remedy. Menyanthes trifoliata 30c was prescribed as an individualised homoeopathic medicine on the basis of symptoms followed by M. trifoliata 200c when the intensity of headache increased. The patient improved symptomatically as evidenced by relief in headache and visual blurring; the adenoma shrank from 1.0 × 1.3 × 1 cm to 3.3 × 4.1 × 2.9 mm. Homoeopathic remedies are helpful in PAs to reduce tumour size and relieve symptoms.
Keywords
Pituitary macroadenoma
Menyanthes trifoliata
Boericke’s repertory
Homoeopathy
Homoeopathic medicine

INTRODUCTION
Pituitary adenomas (PAs) are usually slow growing and non-malignant, but represent a major burden to patients and health-care systems. They are classified based on size into microadenomas, macroadenomas and giant tumours. PAs can be further classified into functional and nonfunctional adenomas based on their hormonal activity in vivo. Functioning PAs cause increased secretion of one or more anterior pituitary hormones, whereas non-functioning adenomas may compress the surrounding anterior pituitary areas, resulting in hormone deficiency.[1] PA accounts for 10% of all central nervous system tumours; it is the third most common tumour. The worldwide prevalence of PAs is approximately 17%.[2] In a meta-analysis, the incidence of PAs averaged 16.7% in general, 14.4% on autopsy and 22.5% on radiological examination.[3] The appearance of PAs depends on tumour size and functional status. Approximately two-thirds of PAs may secrete excess hormones. Visual disturbances, headache and hormone deficiency may be caused by the mass effect, while acromegaly or Cushing’s disease may occur in functioning or secreting adenomas. Based on the most recent literature, mortality in patients with nonfunctional PA is increased, with survival being more compromised possibly in women and patients diagnosed at an older age.[4]
Trans-sphenoidal surgical adenoma resection is the initial treatment option for all tumours except prolactinomas. Radiation is reserved for patients in whom tumour size, hormone levels or both cannot be adequately reduced after surgery, drug therapy or both.[1,5] There are published case reports on PAs showing promising results when treated with homoeopathy.[6-8]
Individualised homoeopathy, based on the principle of symptom similarity, can offer treatment options and is without adverse effects.[9] A recent search on the PubMed database with search term ‘homoeopathy AND pituitary adenoma’ after applying filters – article types (case reports, clinical study and clinical trials); text availability (abstract, free full text and full text) and publication dates (from 1940 to 2023) – revealed only one case report. Therefore, the present case study of pituitary macroadenoma responding to individualised homoeopathic treatment can add to the existing knowledge base.
In this manuscript, we present a case on pituitary macroadenoma successfully treated with single homoeopathic medicine, following the basic principles of homoeopathy. The case was repertorised using O. E. Boericke’s repertory according to the 4th method of repertorisation[10] to confirm the homoeopathic remedy.
CASE REPORT
Patient information
A 38-year-old woman who was a civil engineer by profession presented to the outpatient department on 19 February 2020 with headache, occasional blurred vision and sensation of heat on the vertex for 7 years.
History of the present complaints
The patient was apparently well 7 years back; she started experiencing headache only in the evening hours for 3–4 days in a week and which was ameliorated by sleep. Gradually, the intensity and frequency of the pain increased for which she started taking painkiller (Disprin) on her own, which temporarily ameliorated the suffering. The pain extends over the left parietal region to the frontal and occipital regions and has a throbbing character with a feeling of heaviness. The pain is triggered by climbing stairs and relieved by external pressure. She consulted for allopathic treatment (gabapentin) but that provided temporary relief. Four weeks later, she was advised to undergo magnetic resonance imaging (MRI) of the brain (plain and with contrast) which revealed a pituitary macroadenoma. She stopped allopathic treatment and switched to homoeopathy.
Personal history
She had a history of recurrent urinary tract infections; she underwent a cholecystectomy for gallstones 4 years prior.
Generals
She had a body mass index of 25 kg/m2. Menses were regular with last menstrual period 30 January 2020 and no other associated complaints. She craves meat and fish, has low thirst, always has icy cold extremities and thermal reaction chilly. The mental generals were not significant to be considered for selection of similimum.
Clinical findings
Physical examination revealed no evidence of neurological deficit resulting from the tumour, normal blood pressure (124/82 mm Hg) and normal pulse rate (80 beats/min).
Diagnostic assessment
Endocrinological screening which includes S. cortisol, S. prolactin and thyroid profile was within normal limits. MRI brain (plain and contrast) revealed 1.0 × 1.3 × 1 cm (anteroposteriorly × transversely × craniocaudally) pituitary macroadenoma with no extensions [Figure 1].
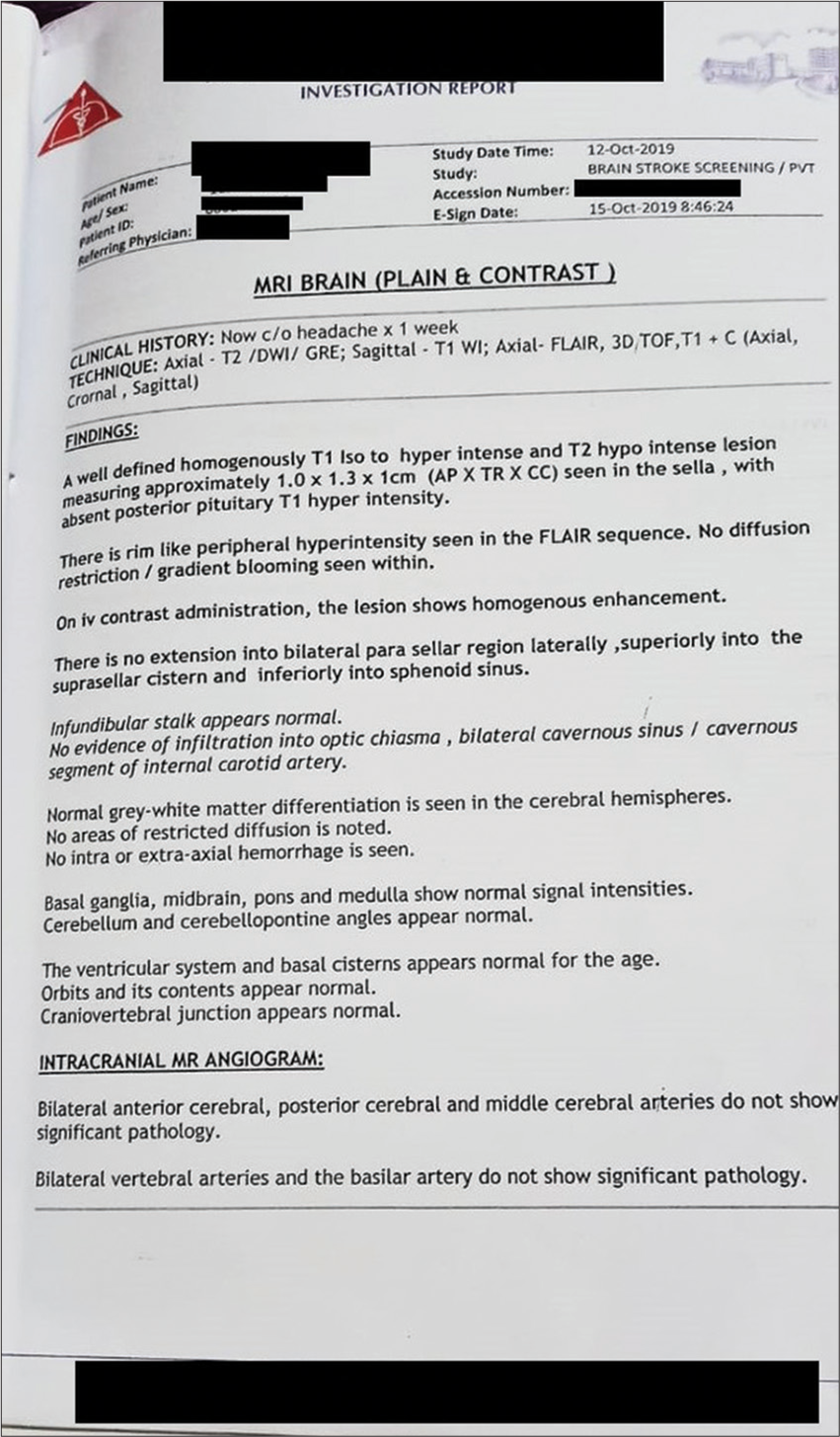
- Magnetic resonance imaging report done in 2019.
Repertorisation
As the generals were lacking, the case was repertorised with O. E. Boericke’s repertory using the Hompath Firefly App by Hompath, Mumbai, India (version: 5.0.0). The six medicines with maximum score in descending order were as follows: Belladonna, Pulsatilla, Cinchona, Gelsemium, Menyanthes and Nux m [Figure 2].
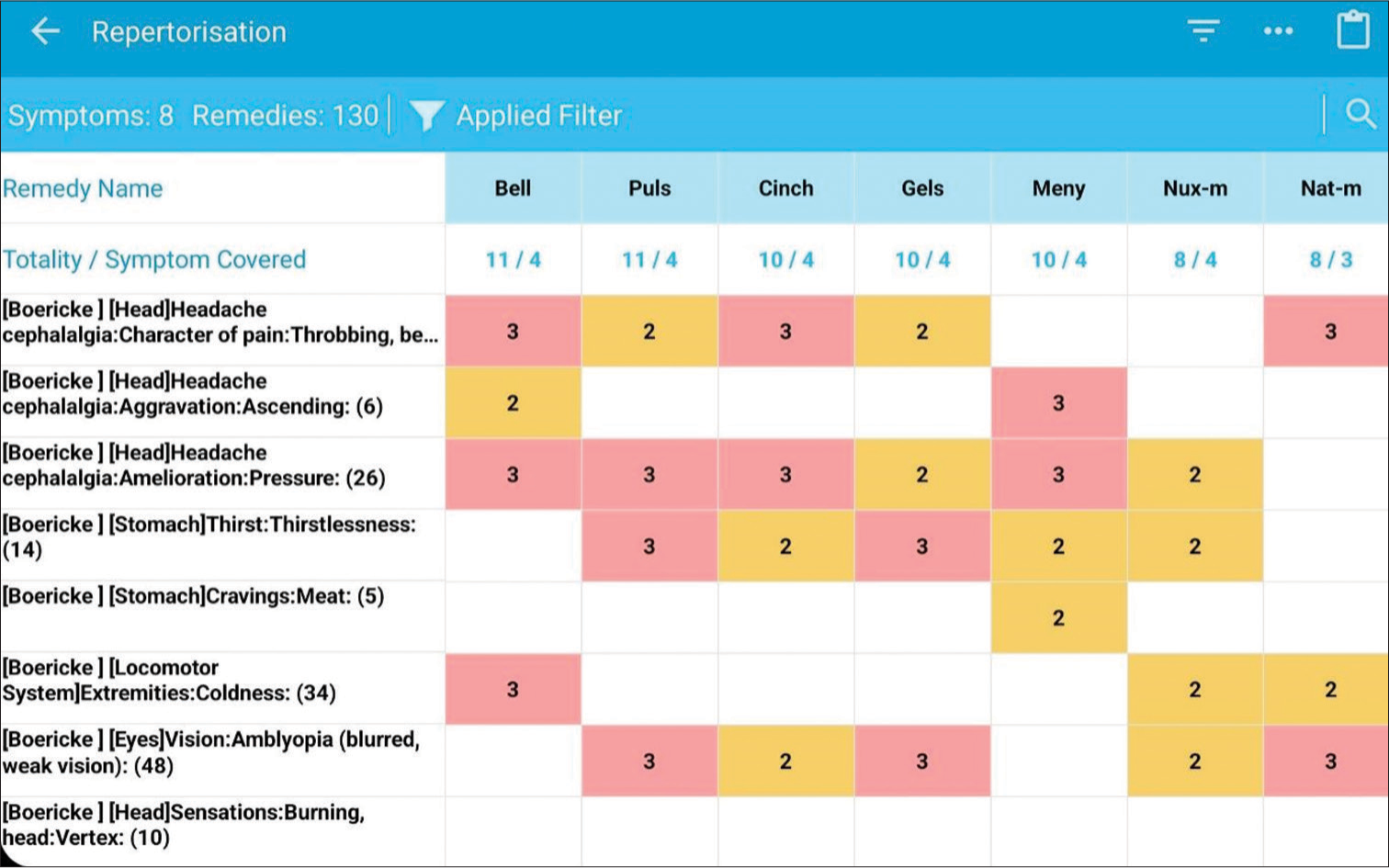
- Repertorisation sheet, Pink: First Grade, Yellow: Second Grade.
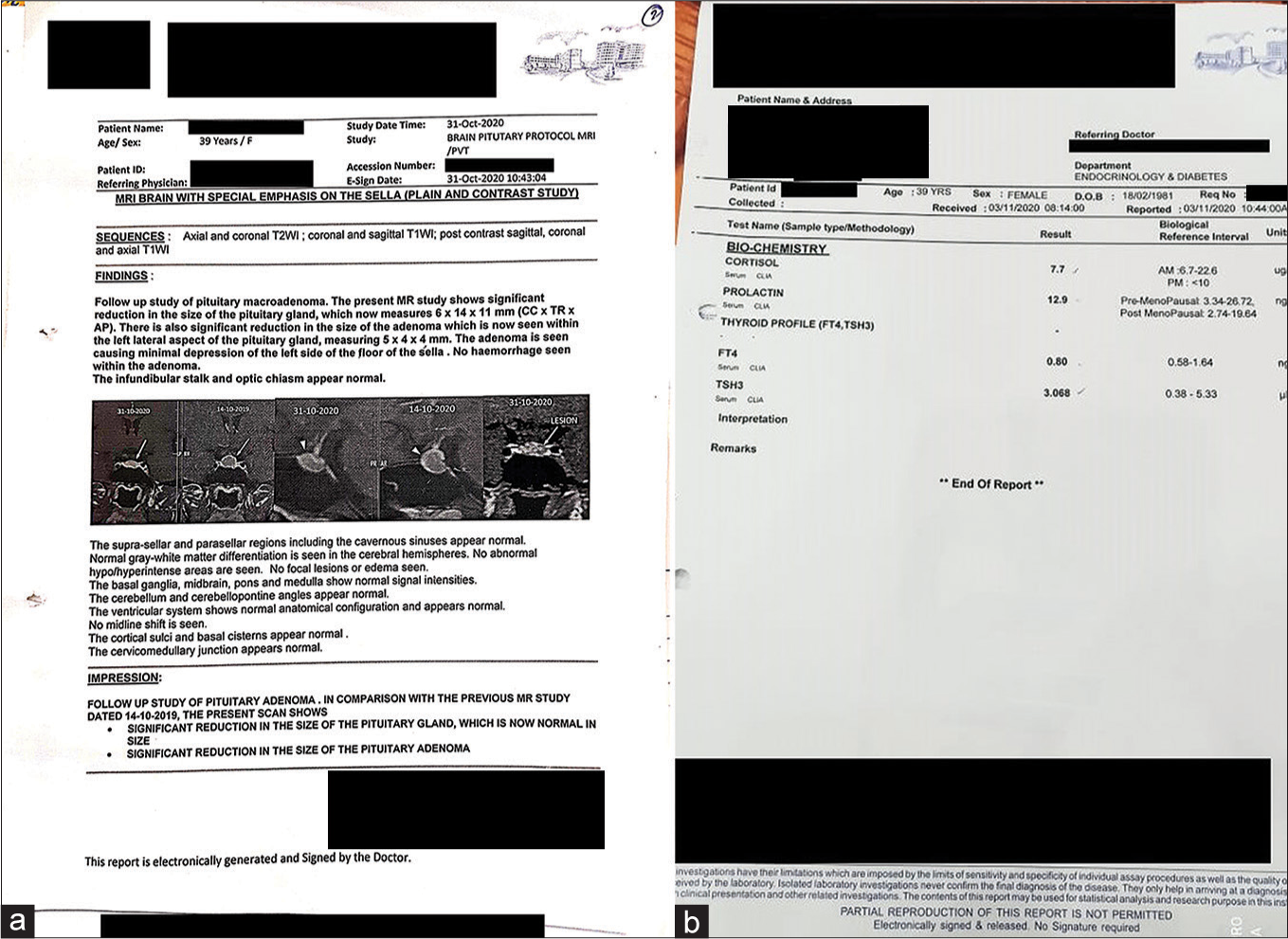
- (a) Magnetic resonance imaging report done in 2020. (b) Hormonal profile.
Therapeutic intervention
After referring to various Materia Medicas,[11-16] the prescription was selected. The maximum symptoms of the case matched with Menyanthes trifoliata, so 30C was prescribed.
Follow-up
During the follow-up [Table 1] over 2 years, significant improvement was noticed in symptomatology as well as in radiology reports. M. trifoliata 200C was prescribed when the intensity of headache increased. Therapeutic lifestyle changes were recommended, including the practice of yoga.
| Follow-up date | Complaint | Investigation | Medicine prescribed |
|---|---|---|---|
| 19/02/2020 (First visit) | Throbbing headache with feeling of heaviness and blurring of vision | (12/10/2019) MRI Brain (Plain and contrast) revealed 1.0×1.3×1 cm (anteroposteriorly×transversely× craniocaudally) pituitary macroadenoma with no extensions |
1 . M. trifoliata 30C twice a day for 2 days. 2. Placebo, twice a day for 1 month |
| 03/04/2020 | The intensity of headache was reduced. Patient was much better |
– | Placebo, twice a day for 1 month |
| 08/06/2020 | Patient was much better. No blurring of vision | –2 | Placebo, twice a day for 1 month |
| 10/08/2020 | Intensity of headache↑ No blurring of vision | – | 1. M. trifoliata 200C once a day for 2 days 2. Placebo, twice a day for1 month |
| 30/11/2020 | Patient was much better | (3/11/2020) [Figure 3] S. Cortisol-7.7 mcg/dL S. Prolactin-12.9 ng/mL Thyroid profile FT4-0.80 ng/dL TSH-3.06 mU/L (31/10/2021) MRI brain: Significant reduction in size in comparison to previous scan • Significant reduction in the size of pituitary gland, which is now normal in size • Significant reduction in the size of the PA, now measuring 5×4 × 4 mm |
Placebo, twice a day for 1 month |
| 22/03/2021. | Complaints of slight aggravation Headache slightly ↑ | - | 1. M. trifoliata 200C once a day for 2 days. 2. Placebo for 1 month |
| 24/08/2021 | Headache relieved considerably Pain in cervical region | (08/11/2021) Contrast-enhanced MRI brain: Pituitary gland normal in size [Figure 4] A small (3.3×4.1×2.9 mm) non-enhancing lesion in the left lateral aspect of the gland |
1. Placebo, twice a day for 1 month 2. Cimicifuga 30C, twice a day for 2 days. |
MRI: Magnetic resonance imaging, PA: Pituitary adenoma, TSH: Thyroid-stimulating hormone, FT4: Free thyroxine, S. cortisol: Serum cortisol, S. prolactin: Serum prolactin, M. trifoliate: Menyanthes trifoliate
The possible causal attribution of the treatment outcome was assessed using the modified Naranjo criteria as proposed by the Homoeopathic Pharmacopoeia Convention of the United States clinical data working group[17,18] [Table 2]. The score obtained (09) reflects the probability that the improvement in the patient can be attributed to the homoeopathic medicine administered.
| S. No. |
Yes | No | Not sure or N/A |
|
|---|---|---|---|---|
| 1. | Was there an improvement in the main symptom or condition for which the homoeopathic medicine was prescribed? | +2 | 0 | 0 |
| 2. | Did the clinical improvement occur within a plausible time frame relative to the drug intake? | +1 | 0 | 0 |
| 3. | Was there an initial aggravation of symptoms? | 0 | 0 | 0 |
| 4. | Did the effect encompass more than the main symptom or condition, that is, were other symptoms ultimately improved or changed? | +1 | 0 | 0 |
| 5. | Did overall well-being improve? (in ORIDL Scale) | +1 | 0 | 0 |
| 6. | A. Direction of cure: do some symptoms improve in the opposite order of the development of symptoms of the disease? | 0 | 0 | 0 |
| B. Direction of cure: do at least two of the following aspects apply to the order of improvement of symptoms? • From organs of more importance to those of less importance • From deeper to more superficial aspects of the individual • From the top downwards |
0 | 0 | 0 | |
| 7. | Do ‘old symptoms’ (defined as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? | 0 | 0 | 0 |
| 8. | Are there alternate causes (other than the medicine) that-with a high probability-could have caused improvement? | 0 | +1 | 0 |
| 9. | Was the health improvement confirmed by any objective evidence? (e.g., laboratory test, clinical observation) | +2 | 0 | 0 |
| 10. | Did repeat dosing, if conducted, create similar clinical improvement? | +1 | 0 | 0 |
ORIDL: Outcome in relation to impact on daily living, N/A: Not applicable
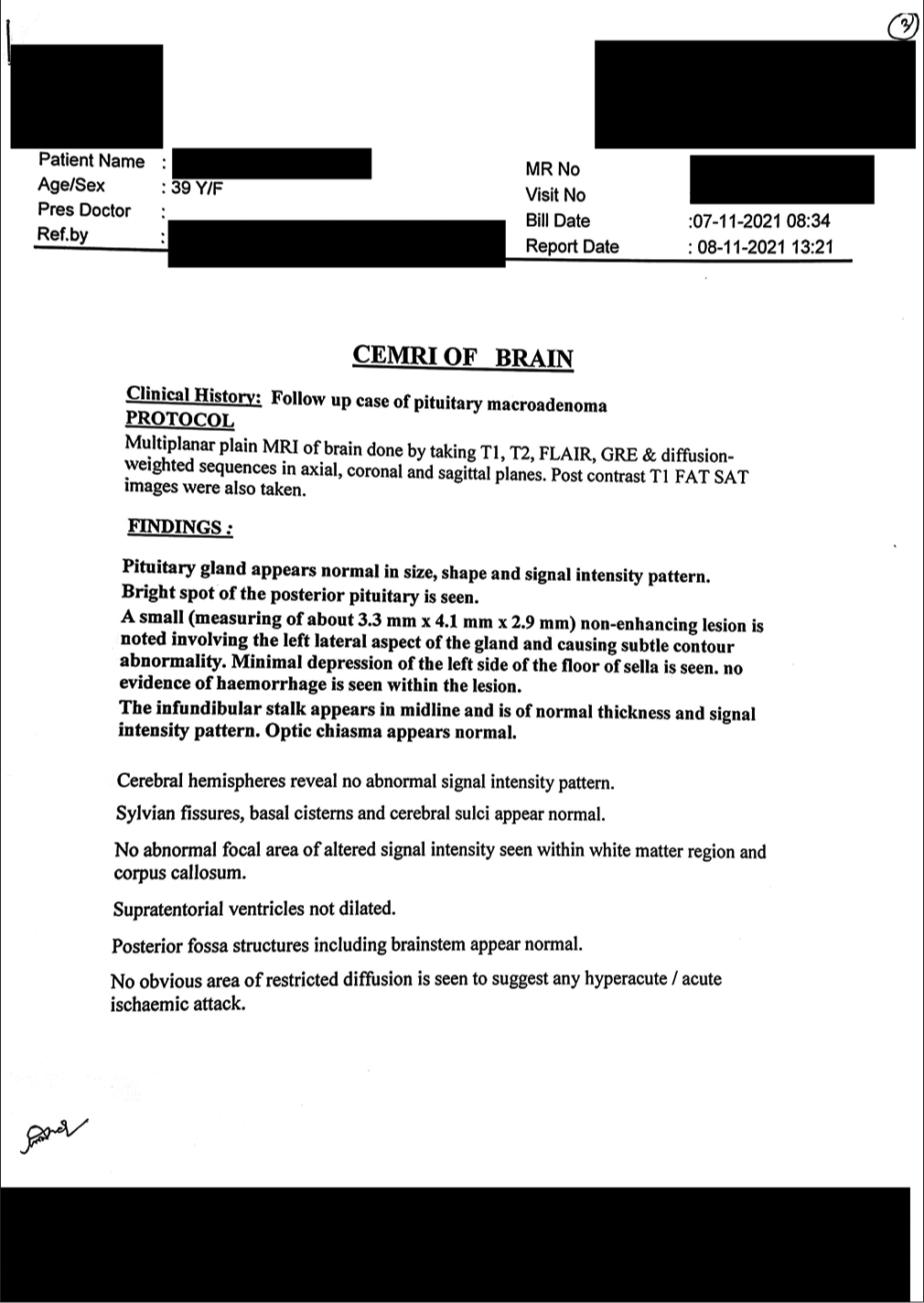
- Magnetic resonance imaging report done in 2021.
DISCUSSION
Homoeopathy is a system of medicine that focuses on treating patients holistically. In homoeopathy, detailed case taking is done to understand the patient’s constitution, and a single remedy is chosen on the basis of totality of symptoms.
This case report suggests the positive role of homoeopathic medications in reducing the size of PAs along with improvement in the patient’s symptoms. Reporting of the case adhered to the HOM-CASE-CARE[18] guidelines.
The case reports published earlier have shown the effectiveness of individualised homoeopathy in the treatment of PAs and its complications.[6-8]
While homoeopathic treatment has shown favourable results in this case, controlled studies with long-term follow-ups and large sample sizes are required for validating the effects of homoeopathic treatment.
CONCLUSION
Homoeopathic remedies are helpful in PAs and can reduce the size of the tumours along with improvement in the symptoms. As the generals were lacking, the case was repertorised using O. E. Boericke’s repertory which highlights the role of clinical repertories in practice. The results of this case study warrant a rigorous trial to test the efficacy of homoeopathic interventions in PAs.
Ethical
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Pituitary adenoma In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554451/ [Last accessed on 2021 Nov 16]
- [Google Scholar]
- The prevalence of pituitary adenomas: A systematic review. Cancer. 2004;101:613-9.
- [CrossRef] [PubMed] [Google Scholar]
- Mortality in patients with non-functioning pituitary adenoma. Pituitary. 2018;21:203-7.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis and treatment of pituitary adenomas: A review. JAMA. 2017;317:516-24.
- [CrossRef] [PubMed] [Google Scholar]
- Homoeopathic treatment of pituitary adenoma: A case report. Malays J Med Biol Res. 2020;7:67-86.
- [CrossRef] [Google Scholar]
- Pituitary microadenoma treated with individualized homeopathic medicine: A case report. Homeopathy. 2020;109:243-7.
- [CrossRef] [PubMed] [Google Scholar]
- Two cases of pituitary tumor. 2013. India: Hpathy Medical Publishers; Available from: https://hpathy.com/clinical-cases/two-cases-of-pituitary-tumor [Last accessed on 2021 Nov 16]
- [Google Scholar]
- Do homeopathic medicines provoke adverse effects? A systematic review. Br Homeopath J. 2000;89(Suppl 1):S35-8.
- [CrossRef] [PubMed] [Google Scholar]
- Keynotes and characteristics with comparison of some of the leading remedies of the Materia Medica with bowel nosodes In: 15th impression. New Delhi: B Jain Publishers Pvt Ltd.; 2016.
- [Google Scholar]
- Keynote to the Materia Medica as taught by Henry N. Guernsey Philadelphia, PA: Hahnemann Publishing House; 1887.
- [Google Scholar]
- A synoptic key to the Materia medica including brief repertory In: 3rd Impression (1st ed). New Delhi: B. Jain Publishers Pvt Ltd.; 2011.
- [Google Scholar]
- A dictionary of practical materia medica In: 33rd Impression. New Delhi: B. Jain Publishers Pvt Ltd.; 2017.
- [Google Scholar]
- Boericke's new manual of homoeopathic Materia Medica with repertory In: 3rd Revised and augmented edition based on 9th edition. New Delhi: B. Jain Publishers Pvt Ltd.; 2011.
- [Google Scholar]
- A handbook of Materia Medica and homoeopathic therapeutics Philadelphia, PA: F.E. Boericke; 1889.
- [Google Scholar]
- A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239-45.
- [CrossRef] [PubMed] [Google Scholar]
- Homeopathic clinical case reports: Development of a supplement (HOM-CASE) to the CARE clinical case reporting guideline. Complement Ther Med. 2016;25:78-85.
- [CrossRef] [PubMed] [Google Scholar]




