
Translate this page into:
Challenges faced in homoeopathic treatment in autism – A case series
*Corresponding author: Dr. Swapna Kamath, M.D. (Hom) Psychiatry, Department of Psychiatry, Ira Gurukul and Vishesh Child Development Centre, Kush Regency, Post Office Lane, Behind Apna Bazaar, Andheri West, Mumbai, Maharashtra, India. skamath25@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Kamath S. Challenges faced in homoeopathic treatment in autism – A case series. J Intgr Stand Homoeopathy 2021;4(1):29-36.
Abstract
Objectives:
Autism spectrum disorder (ASD) is one of the most puzzling and complex of the neurodevelopmental disorders, especially regarding its diagnosis and management. The objective of this study was to achieve an in-depth understanding of the various challenges faced by a homoeopath and how homoeopathy is to be used conjointly with other ancillary measures in managing ASD. The case series highlights these and presents an integrated understanding of various concepts required by a homoeopath in effectively managing children with ASD.
Materials and Methods:
Detailed histories of the two cases were taken from the caregivers. Both patients were also observed in their day-to-day functioning, at school and during therapies. This further contributed to the early detection and diagnosis, planning appropriate management strategies, assessing the action of the selected remedy and deriving inferences. Homoeopathic treatment was used along with the required ancillary measures.
Results:
The challenges in managing the cases were mainly with respect to formulating a diagnosis, understanding the importance of disease evolution, differentiating between the common and the characteristic symptoms of the disease, application of homoeopathic principles and arriving at a similimum. On reflection, it showed the value of using the bio-psychosocial model to highlight the relationships among the different forces, determine the evolution in individual cases and emphasise the need for holistic intervention. The importance of a sound knowledge of the principles of homoeopathy and their correct application to arrive at a similimum was also learnt through reviewing the results of intervention. Further, the results showed that homoeopathy along with ancillary measures helped to bring about a significant change in functioning on all fronts and a better adaptation of the children to their environments.
Conclusion:
Homoeopathic intervention in children with autism holds a promise. Integration with ancillary measures enhances the outcome. Homoeopaths would need to train themselves in applying the bio-psychosocial model and integrating it with homoeopathic principles to ensure a favourable outcome. The findings of this study can provide important leads for professionals involved in the care of children with ASD and the affected families.
Keywords
Autism spectrum disorder
Autism and challenges
Ancillary measures
Bio-psychosocial model
Homoeopathy and autism treatment

INTRODUCTION
Autism and clinical presentation
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterised by impaired social interaction, deficits in verbal and non-verbal communication and restricted or repetitive behaviours or unusual or severely limited interests.[1] Characterisation as a ‘spectrum disorder’ conveys that a wide variation exists in the type and severity of symptoms experienced – no two children appear or behave the same way. Symptoms can range from mild to severe and often change overtime. It is estimated that globally around 62 people/10,000 are affected with autism.[2] Since ASD represents itself within its wide spectrum of symptoms and severity, recognising symptoms and establishing a diagnosis can be challenging.
Arriving at the diagnosis using clinical acumen and reliable diagnostic tools is very important in cases of autism. A detailed developmental history, neurodevelopmental examination, vision and hearing testing can help the homoeopath to formulate the diagnosis and rule out the comorbidities, if any. The Childhood Autism Rating Scale (CARS), Indian Scale for screening of Autism, Vineland Social maturity Scale (VSMS) and M Chat are some of the few scales used for assessing patients.
To the best of our knowledge, no specific medication exists to treat autism. The pharmacological approach is addressed to manage the symptoms of hyperactivity, maladaptive behaviour patterns, aggression and self-injurious behaviour, anxiety and sleep disturbances or to manage comorbidities like epilepsy. The general principles for pharmacotherapy in ASD are similar to the other neuropsychiatric conditions.[3] Conventional medications include psychoactive drugs, anti-depressants, anti-psychotics, anti-epileptics and stimulants. These medicines have their own side effects and should be used after weighing their pros and cons with the physician.
A multimodal and integrative approach will help children with autism to reach an optimal level of functioning. A systematic Individualised Education Programme[4] focussing on sensory integration, occupational therapy, speech therapy, special education, behaviour therapy, social skills training and vocational training is the mainstay in managing this condition.
How can homoeopathy help children with autism to reach their optimal level? What are the various challenges likely to be encountered by a homoeopath in the treatment of such a complex neurodevelopmental disorder?
Autism is a multi-factorial phenomenon where in the biological, psychological, psychodynamic and maternal state during pregnancy, can contribute to its emergence and maintenance. Approaching a case with the understanding of the bio-psychosocial model[5] complements homoeopathic treatment, as they both focus on holistic well-being of an individual. Just like homoeopathy, this model maintains that health and illness are caused by multiple factors, the mind and body cannot be distinguished in matters of health or illness.
The challenges can start from early recognition of symptoms to arrive at the diagnosis, ruling out the comorbidities and planning therapeutic interventions.[6] One has to understand the changes in symptomatology over phases of development as well as because of the therapies. Despite being fully trained in the art of case taking, it is easy for a homoeopath to get lost in the maze of complex symptoms and prescribe a remedy on the myriad clinical presentations, confusing them for qualified mental symptoms. Hence, differentiating between the common and the individualistic symptoms of a case is essential. Sound grounding in homoeopathic philosophy and its application along with knowledge of obstacles to recovery in every case helps. An additional task is formulating a general plan of treatment in the form of therapeutic intervention and integrating with the indicated multiple modalities.
MATERIALS AND METHODS
The two children were evaluated based on signs and symptoms and their observations in an inclusive setting. The diagnosis was confirmed using the CARS, VSMS and receptive and expressive language scale (REELS). The cases were defined taking inputs from their parents, teachers and therapists’ observations and general observations made by the physician. The expressions at the physical, mental and behavioural level were noted along with their intensity and characteristic nature.
The study design was a retrospective case study from the author’s database of homoeopathic case studies of children with ASDs. The setting is private practice of the author.
Both the cases provided good learning and they highlighted the challenges in treating autism. The cases emphasised the need to have a sound knowledge of the principles of homoeopathy and its application along with clinical understanding. The responses to intervention were evaluated and the follow-up criteria were also set.
Illustrative cases
Case 1
Mast AP, an 8-year-old boy, is studying in an inclusive school for children with special needs for 2 years. He is short tempered and deliberately breaks things – especially others’ favourite belongings. He would refuse to go for therapy at times, if forced would fling things. He was hyperactive, always moving about, sitting tolerance around 10–15 minutes. He refused eye contact and preferred solitary play. He exhibited stereotypes in the form of hand flapping and rubbing his genitalia. His sensory concerns included sensitivity to cooker whistles and fire crackers. He did not like to read and write and his comprehension was poor. There was no reciprocity and his speech was need based.
The child was on occupational therapy and speech therapy since enrolling in the school. His day-to-day functioning had started becoming difficult at school and the therapists were finding it difficult to work with him due to his anger and lashing out during therapy.
This resulted in discussion with his parents and the need to start medications for the child. His parents agreed to homoeopathic treatment, which led to further case details.
Mast AP was a full-term normal baby, with normal birth weight and no significant birth history. The motor milestones were normal, speech was delayed. No significant birth or pregnancy history was obtained. He was diagnosed at the age of 4.5 years. He started schooling at 6 years of age.
There was no significant family and personal medical history.
Physical generals
Appetite: Low, fussy eater
Thirst: Normal
Thermals: Chilly
Cravings: Vada Pav (potato fritter) would get it in his tiffin daily and would refuse to eat anything else
Aversion: Nothing specific
Sleep: Stays awake till 2–3 am daily, difficulty in falling asleep on days when there have been a lot of events
Perspiration: Scanty
Urine: Normal
Stool: Constipated, has to strain
TEST SCORES: CARS 35 (mild degree of autism)
VSMS: 60: Mild retardation in social functioning
BERA: NORMAL, REELS (Expressive speech – 34–36 months).
Totality
Anger violent++
Anger destructive++
Striking++
Malicious++
Jealousy++
Restless++nervousness tendency to
Noise agg sensitive too
Comprehension difficult
Gestures automatic
Handling genitalia
Cr fried food, spicy food
Stools constipation
Sleeplessness++
Chilly.
Result of Repertorisation [Figure 1]

- Rubrics selected for repertorization
Nux vomica: 18/8, Hyoscyamus niger: 12/7 and Tarentula hispanica: 12/7.[7]
Remedy differentiation [Table 1]
| Tarentula hispanica | Hyoscyamus niger | Nux vomica | |
|---|---|---|---|
| Family | Animal kingdom: The Spanish spider acts on the nervous system. There is excess energy. Must keep themselves busy. |
Plant kingdom: Henbane Acts on the mind, brain and nervous system. |
Plant kingdom: Strychnine: Acts on the nervous system Over sensitiveness. |
| Anger | Hateful, destructive, rolls on the ground or strikes vehemently, rolls his head and rubs it to relieve distress. | Acute mania, worse from emotions, jealousy, fright. Rage, desire to strike, bite, fight, insult, scold and kill. | Violent Anger, Quick to act. Desire to strike, spiteful. |
| Behaviour | Hurried, restless, impulsive, exhibits physical activity, cannot keep quiet in any position>rubbing surfaces. Good sense of Rhythm, inclination to dance>music Excited with bright colours Immoral, selfish, cunning, malice, mischievous Feigning all the time. | Restless, fidgety, beats others, violent, poor impulse control Talks, talking non-sense, makes gestures, laughs, foolish behaviour. | Restlessness, fidgetiness, < mental exertion, aversion to work Fault finding, reproaches others Head strong, self-willed. |
| Affections | Chorea, hysteria, spinal irritability. | Convulsion, fever | Sleeplessness excitement from. Digestive system affections, constipation. |
All the three remedies act on the nervous system and exhibit destruction, hyperactivity and impulsivity. However, the physical symptoms of sleep disturbance and constipation were predominantly covered by N. vomica and hence it was prescribed.[8]
Miasmatic understanding: Sycotic. Susceptibility assessment
Qualified mental characteristics
High sensitivity
Good vitality
Hence, the susceptibility falls under moderate to high zone.
Hence, N. vomica 200 was prescribed.
Follow-ups [Table 2]
| Follow-ups | With therapy | With homoeopathy | |
|---|---|---|---|
| First 3 months N. vomica200 single dose/weekly. | Behaviour: 1.Anger, impulsiveness, throwing things reduced 2.Restlessness reduced Higher functions: 1.Attention Span: Improved. Sitting tolerance improved: 15–20 min 2.Comprehension improved. Refuses to write 3.Sensory concerns: 1. Stimming – reduced Generals: 1.Appetite/sleep: Improved 2.Constipation> |
With Occupational Therapy improvement seen in Motor: 1.Tone, strength, endurance 2.Eye hand Coordination improved Higher functions: 1.Eye contact, response to name improved 2.With speech therapy: Need based speech. |
1.Response to therapy improved, he started sitting longer for therapy without threatening and destruction of property. |
| Next 3 months Mast A was put on N. vomica200 three doses/week. | Behaviour: 1. Anger, Impulsiveness, Reduced++ 2. Hyperactivity, restlessness reduced++ Higher functions: 1.Attention span: improved++, sitting tolerance improved – 40 min 2.Comprehension –improvedSensory Concerns- 1. Stimming reduced++ 2.Fondling of genital reduced++ generals – SQ. |
With occupational Therapy: Motor: 1.Tone, Strength, endurance: SQ 2.Sensory concerns were improving: Auditory hypersensitivity and flapping reduced With Special Ed: 1.He started reading and writingspeech therapy: Started speaking in full sentences. |
1.Cognition improved 2.Speech improved 3.Started remedial sessions 4.Compliance and sitting tolerance improved. |
| By 6 months N. vomica200 three doses/week. | Same as above | Same as above | Same as above |
| By 9 months Since there was a plateau seen in the progress, even with therapies being continued, he was shifted to N. vomica1 M single dose/week. | Significant improvement seen in: 1.Behaviour 2.Cognition 3.Sensory Concerns 4.Speech 5.Sleep 6.Constipation. |
1.Compliance in the therapies improved. With occupational therapy: 1.Sensory concerns further reduced 2.Maintains eye contact With Special education: 1.Reading and writing skills improved. With speech therapy 2.Reciprocity improved. |
1.Speech improved 2.Cognition improved 3.Sensory concerns reduced 4.Started participating in group therapy. |
| By 1 year, he was on N. vomica1 M single dose | Marked improvement in areas of Behaviour Cognition Sensory concerns Speech Sleep Constipation Appetite. |
1.The child attends his therapies regularly. 2.He is currently preparing for Level ‘A’ open basic examination. 3.Participation in group therapy has started. |
Improvement seen in the overall development of the child. Autism Treatment Evaluation Checklist showed improvement with homoeopathy. Homoeopathy also augmented the therapeutic interventions which further helped him to integrate in the school setting. |
N. vomica:Nux vomica, SQ: Status Quo
Learning from the case
In this case, the indicated remedy was selected not on the basis of the mental symptoms (which were prominent) but on the characteristic concomitants and physical generals. These were the PQRS (Aph 153)[9] and the key toward individualisation. Hence, a sound knowledge of the principles of homoeopathy helps the homoeopath to overcome the challenges in management of cases of autism.
Children on the spectrum have sensory issues and delayed speech and language development. Regular therapies not only bridge the developmental gaps but also promote cognitive, language, play way and social development. Homoeopathy, along with the abovementioned ancillary measures, helps in the holistic development of the children with autism. Hence, this case also highlighted how an interprofessional collaboration using a multidisciplinary approach in the management of cases on the spectrum helps in improving the effectiveness in the treatment.
Illustrative case no 2
Mast AS, a 4-year-old-male child, was referred to the resource room by his class teacher as the child was unlike other 4 years old in her class. Her primary concern was that he needed assistance for every activity. He responded to his name but did not maintain eye contact. He would not play with his class mates or interact with them. He was very cautious, would avoid playing in the school garden and would not hop or jump. He was restless, would comprehend the questions asked but would not answer. His comprehension was good, concepts were clear and he could remember a lot of details.
On classroom observations and further inquiry with the parents, the following history was obtained.
He would avoid brushing, combing hair, bathing, playing in mud or sand. He could not hold a crayon to scribble or colour. He was a quiet and shy child. He was a quiet and shy child and did not interact with people. He would engage in parallel play but would not establish friendships or conversations during play. He was very sensitive and could not be spoken to loudly. He had to be told to do anything in a low tone of voice. He would stop working if shouted at or pointed out a mistake. There were no temper tantrums.
Birth history
Full term, C section, BCIAB, elderly primipara, gestational diabetes.
Milestones
Motor and Speech mile stones delayed.
The parents were explained about the clinical condition and were asked to get him investigated so that we could take appropriate measures for him at school.
His test scores revealed
BERA: Normal, VSMS: Social Quotient (SQ) was 105 suggesting Average Social Functioning
Meets the DSM 5 criteria for ASD
Gilliam Autism rating scale 3 (GARS 3): Autism index revealed ‘likely’ probability of ASD
ON CONNERS (EARLY CHILDHOOD SCALE): Highest scores were obtained on social functioning and atypical behaviours.
Recommendations by the developmental paediatrician
He would benefit from sensory integration, occupational therapy and group therapy
His parents were keen to start homoeopathy for him, which further led to the following history taking:
Physical generals: P/H: Tendency to catch cold easily with H/O recurrent cold and cough
Appetite: Low, fussy eater, had to be fed.
Thirst: Normal
Cravings: Ice creams, cold drinks but not given as catches cold
Aversion: Nothing specific
Perspiration: Palms, nape of neck while at sleep
Dreams: Frightful wakes up often at night
Thermals: Chilly.
Prescription
The characteristic mental symptoms and physical generals pointed at Silicea, a single dose of Silicea 200 was prescribed. The dose was repeated once in 15 days and then weekly.
The child also started sensory integration therapy with an occupational therapist and was under remediation in the resource room thereby under my observation.
Observations 3 months into Rx (medicines and therapy)
Hyperactivity, restlessness reduced
Sitting tolerance: Improved
Self-help skills: Improving
Fine motor skills: Improving
Gross motor: Started hopping and jumping from height of ½ feet
-
Eye contact: Improving he could maintain it for few seconds.
Sensory concerns remained: SQ
Echolalia: SQ
Dreams: SQ
Cautious behaviour was increasing, scared in doing almost all new activities
Not getting the desired results as per the expectations, the case was reviewed but no major data on the patient was received. Hence, mother’s history during pregnancy was retaken in detail.
History
The mother was a working lady, had a late marriage and a late conception and was not ready for pregnancy. During pregnancy, she would be very angry as her husband would not do any house work and she had to manage both home and work and felt overburdened. At times, she felt lonely and was scared of losing her son due to overwork. She would have frightful dreams almost every night and would sleep with lights on. She constantly wishes she could run away from this. She developed gestational diabetes in the 2nd trimester.
After reevaluation and studying the mother’s mental state during pregnancy, it was inferred that it played a very important role in the genesis of the disease, its manifestation and the outcome. This understanding was highlighted using the bio-psychosocial model [Figure 2].
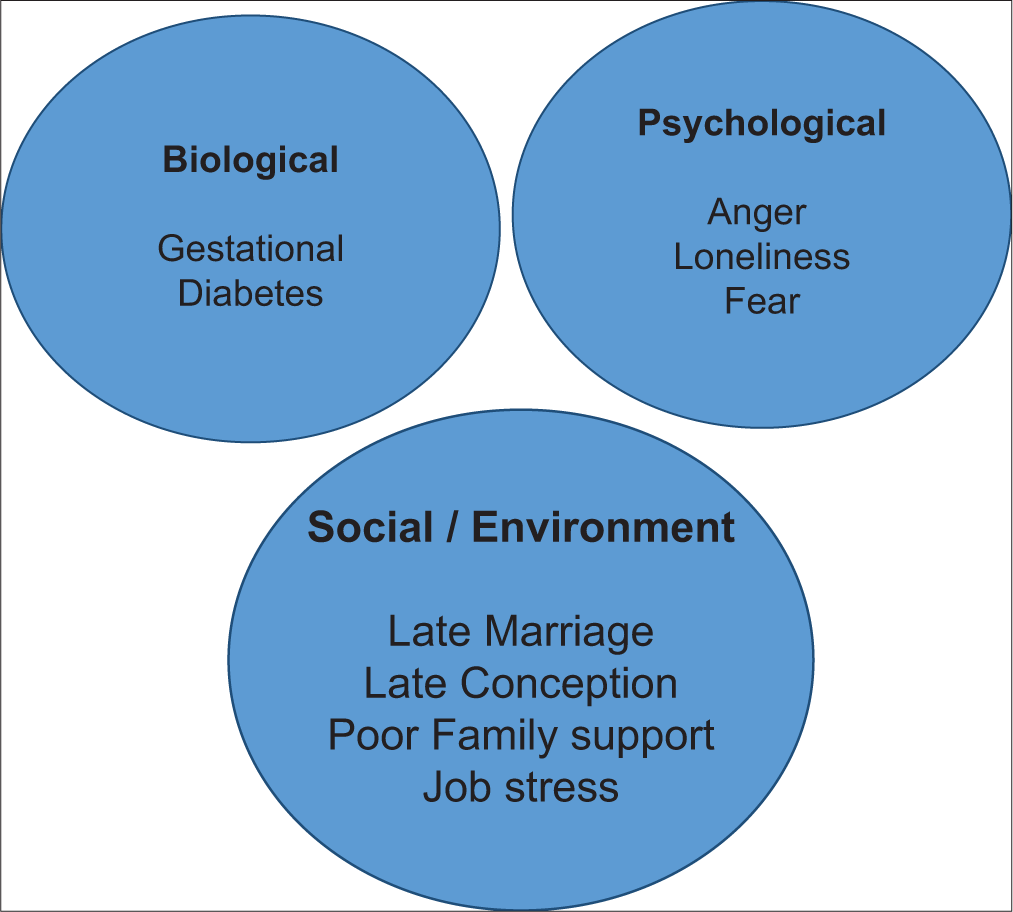
- Understanding the evolutionary totality through the bio-psychosocial model.
The totality was revisited and Stramonium 200[10] single dose was prescribed on the following totality.
Totality
<Dark++
< Solitude ++
Desire Light++
Escape desire to++
Dreams Frightful++
Changes seen
Eye contact: Improved, sustained and maintained
Echolalia: Reduced and reciprocity started developing, play way has improved
Self-expression improved: He would get angry and express his feelings
Dreams: Episodes of waking up in the night reduced considerably
Sleep: Peaceful and sound
Hyperactivity, restlessness reduced
Sitting tolerance further improved
Sensory concerns: Vestibular and proprioceptive concerns, tactile dysfunction – Improved.
Follow-up
Stramonium 200 infrequent repetition and sensory integration therapy followed with remedial education in the resource room.
One year into treatment
On CARS: Mast AS does not meet the criteria for ASD.
Learning from the case:
Early detection and intervention facilitates the sensory, motor and cognitive development, thereby improving the prognosis of the case.
There is an interlink between the bio-psychosocial model and the evolution and manifestation of the illness in an individual. Integrating this model with homoeopathic principles ensures positive outcomes.
Evaluating the case on speculations and guesses before understanding the patient as a whole is being prejudiced and can be misleading. Thus, freedom from prejudice as mentioned by Dr. Hahnemann in Aph 6 is an important learning in the case.
RESULTS AND DISCUSSION
Autism is a multifactorial phenomenon affecting the sensory motor development, perception, language, social skills, cognition and behaviour. The biological, psychological, psychodynamic and maternal state during pregnancy can contribute to the emergence and maintenance of this disorder. The evolutionary history, pre-disposition and dispositional features, helps in perceiving the totality of the case. The two cases highlighted the importance of in-depth knowledge of various concepts required for management of Autism. It helped in the exploration of the bio-psychosocial model, understood the management modalities and relearnt the principles of homoeopathy. It also showed how homoeopathy along with ancillary measures helps to augment the sensory-motor language and cognitive development, thereby bringing out a holistic development and integration of the children in their respective environments.
Both the cases had individualistic presentations and the differentiation between common symptoms of the disease and the characteristic symptom was important in formulating a totality and arriving at a similimum. Case 1 had qualified Mental such as desire to strike, violent anger and destructiveness, with prominent physical generals. It is easy to get carried away and prescribe on striking mental symptoms. However, the lack of any causative factors, evolutionary totality or striking ‘ailments from’ for prescribing demanded an entry through the physical generals which led to the selection of the indicated remedy.
The second case also had characteristic physical and mental symptoms but the selected remedy only gave partial results. Mental state of the mother during pregnancy[11] had a strong impact on the diathesis and thereby the evolution of the disease. The striking metal symptoms such as desire to escape, light desire and dreams frightful helped in selecting the similimum. This led to the unravelling of predisposition and exploration of biological, psychological and social dimension of the illness.
Centesimal scale potencies were utilised in both the cases commencing with 200 C after evaluating the susceptibility. The symptomatology was reviewed periodically with feed backs from the parents and observations of the therapists. When no further improvement was seen, the potency was raised to 1 M in Case no 1. The improvements in both the cases were measured on GARS and Autism Treatment Evaluation Checklist scores indicating a positive outcome of the intervention.
Both the cases highlight how homoeopathy augments the therapeutic interventions which helped the children to integrate in their respective school settings. The use of ancillary measures along with homoeopathy[12] helped to bring about a significant change in prognosis and better adaptation of the children with autism in the environment.
CONCLUSION
For the successful management of cases of autism, it is important to have an in-depth knowledge about the evolution of the disease, its clinical presentation, diagnostic tools, therapeutic interventions and treatment modalities.
Challenges in treatment can be encountered right from early recognition of symptoms, formulating a diagnosis, evaluating the evolutionary history, differentiating between the common and the characteristic symptoms of the disease, application of homoeopathic principles and arriving at a similimum. Addressing these challenges promote awareness, facilitate early diagnosis and improve the quality of care and outcome in Autism.
The bio-psychosocial model complements homoeopathic treatment by helping in understanding the evolution of the disease, patient predispositions and the outcome of the disease.
Early identification, diagnosis and intervention facilitate the sensory-motor-cognitive development, improving the prognosis of the case.
An interprofessional collaboration using a multidisciplinary approach improves the effectiveness of treating children with autism. The therapies help to bridge the developmental gap and promote sensory motor and language development. Homoeopathy along with ancillary measures improves the quality of care and the outcomes in autism.
A sound knowledge of homoeopathic principles and its correct application helps in arriving at a similimum. Homoeopathy has a vast scope in treating autism and the homoeopath can up bridge his knowledge, overcome the challenges and enable holistic development of children with autism.
Scope of Homoeopathy in Treating Autism [Figure 3]. Copyright @drswapnakamath

- Scope of Homeopathy in treating Autism.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- DSM 5-Diagnostic and Statistical Manual Neurodevelopmental Disorders (5th ed). Philadelphia, PA: American Psychiatric Association; 2015. p. :1-2.
- [Google Scholar]
- Global prevalence of autism and other pervasive developmental disorders. Autism Res. 2012;5:160-79.
- [CrossRef] [PubMed] [Google Scholar]
- Autism Spectrum Disorder in Children and Adolescents: Pharmacological Interventions UpToDate; 2020. Available from: https://www.uptodate.com/contents/autism-spectrum-disorder-in-children-and-adolescents-pharmacologic-interventions [Last accessed on 2020 Dec 29]
- [Google Scholar]
- Individual education plan goals and services for adolescents with autism: Impact of age and educational setting. J Spec Educ. 2009;44:146-60.
- [CrossRef] [Google Scholar]
- The clinical application of the biopsychosocial model. Am J Psychiatry. 1980;137:535-44.
- [CrossRef] [PubMed] [Google Scholar]
- Autism spectrum disorders: Early detection, intervention, education, and psychopharmacological management. Can J Psychiatry. 2003;48:506-16.
- [CrossRef] [PubMed] [Google Scholar]
- The Principles and Art of Cure by Homoeopath (3rd ed). New Delhi: B. Jain Publisher Private Ltd.; 2018.
- [Google Scholar]
- Repertory of Homeopathic Materia Medica. 2004. (6th ed). New Delhi: B. Jain Publisher; Available from: http://homeooint.org/books/kentrep/index.htm [Last accessed on 2020 Dec 29]
- [Google Scholar]
- Materia Medica of Homoeopathic Remedies (2nd ed). New Delhi: B. Jain Publishers Private Ltd.; 1999.
- [Google Scholar]
- Antenatal maternal anxiety and stress and the neurobehavioural development of the fetus and child: Links and possible mechanisms. A review. Neurosci Biobehav Rev. 2005;29:237-58.
- [CrossRef] [PubMed] [Google Scholar]
- Healing Autism with Homeopathy in Synergy with Other Therapies. 2015. Hpathy Ezine. Available from: https://www.hpathy.com/material-medica/healing-autism-with-homeopathy-in-synergy-with-other-therpaies
- [Google Scholar]




